










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.2 Lima abr-jun 2021
http://dx.doi.org/10.25176/rfmh.v21i2.3708
Original article
Platelet / spleen ratio for the diagnosis of esophageal varices and the risk of bleeding in patients with liver failure
1Unidad Médica de Alta Especialidad Hospital de Especialidades, Centro Médico Nacional “Gral. de Div. Manuel Ávila Camacho”, Instituto Mexicano del Seguro Social, Puebla-Puebla México.
2Unidad de Medicina Familiar n°8, Delegación Puebla, Instituto Mexicano del Seguro Social. Puebla, Puebla-México.
3Hospital General de Zona número 20, Delegación Puebla, Instituto Mexicano del Seguro Social, Puebla-Puebla, México.
4Hospital General de Zona n° 1, Tepic, Nayarit-México.
5Escuela de Medicina, Universidad Anáhuac Campus Norte, Estado de México-México.
Introduction:
Upper gastrointestinal bleeding of variceal origin has a high mortality. The platelet count/spleen major diameter ratio may be a useful noninvasive parameter to predict esophageal variceal bleeding in cirrhotic patients
Objective:
To determine the sensitivity and specificity of the platelet count/spleen diameter ratio for the diagnosis of esophageal varices with risk of bleeding in patients with hepatic insufficiency.
Material and Methods:
Process study, performed in a Second Level Medical Facility, in patients with liver failure who underwent ultrasound, blood cytometry, liver function tests and endoscopy. Sensitivity and specificity of the platelet/spleen ratio were assessed in patients with esophageal variceal and bleeding risk.
Results:
There were 70 patients: 28 women, 42 men; main cause of liver failure in men was ethylism in 31 patients and hepatitis C virus in 20 women. The spleen-platelet ratio has a sensitivity of 90%, specificity 83%, false positives 16%, false negatives 9%, positive predictive value 94%, negative predictive value 75%, prevalence of 74% and diagnostic accuracy of 88% to diagnose esophageal varices with risk of bleeding.
Conclusion:
Platelet/spleen ratio is a useful, non-invasive study to diagnose esophageal varices with bleeding risk, in hospitals where endoscopy is not available.
Key words: and Gastric Varices; Gastrointestinal Hemorrhage; Hepatic failure; Hepatic Insufficiency; Diagnosis. (source: MeSH NLM).
INTRODUCTION
Portal hypertension is the increase of portosystemic pressure in any segment of the portal venous system, caused by pre-hepatic or post-hepatic alterations or by other causes1. It occurs when the portocaval gradient is higher than 5 mmHg and is the most frequent and studied cause of hepatic cirrhosis. From 5 to 33% of these patients have varices, which may appear at any part of the gastrointestinal tract, the most frequent site being the distal centimeters of the esophagus. The presence of varices is correlated with the severity of liver disease1,2. The hepatic venous pressure gradient is the ratio between portal pressure and vena cava pressure and predicts the appearance of varices. Clinically significant portal hypertension is 10 mmHg, and is a prognosis factor in patients suffering from portal hypertension1.
When the gradient reaches 12 mmHg, variceal hemorrhage occurs. The main risk factors are: international normalized ratio (INR) greater than 1.5, portal vein diameter greater than 13 mm, and thrombocytopenia. When the patient has one or more of these conditions, it is necessary to perform upper gastrointestinal endoscopy to look for varices and to perform primary prophylaxis against bleeding in cirrhotic patients1-3.
In upper gastrointestinal bleeding (UGH), endoscopy has a high sensitivity and specificity in locating and identifying lesions that cause bleeding. In addition, it offers the possibility of a therapeutic approach and primary prophylactic treatment2,4,5.
Certain noninvasive tests are useful in detecting patients at risk of esophageal varices. These include platelet count, splenomegaly, portal vein diameter greater than 13 mm by abdominal ultrasound and lately elastography. However, none of these tests has diagnostic accuracy for large esophageal varices1,6,7.
The platelet count/spleen bipolar diameter (P/B) ratio of less than 909 is a non-invasive parameter that predicts the presence of esophageal varices in cirrhotic patients8. It can be a diagnostic and follow-up alternative to endoscopy, which is expensive and difficult to access, and may be contraindicated in some patients8,9.
The objective was to determine the sensitivity and specificity of the platelet count/spleen major diameter (P/B) ratio for the diagnosis of esophageal varices with risk of bleeding in patients with liver failure.
The study
A cross-sectional study was carried out in which a test of a test was performed in a secondary-level hospital of Instituto Mexicano del Seguro Social (IMSS) (IMSS) in Puebla, Mexico. Patients with liver failure of any degree of severity, of both sexes, over 18 years of age and who agreed to participate in the study by filling out and signing an informed consent form were included; patients with acute liver failure and those who died during the study were excluded.
Liver failure was defined by the presence of an INR >1.5, increased aminotransferases, anemia, leukopenia, hypoalbuminemia, and liver disease manifested by anorexia, weight loss, weakness, fatigue, osteoporosis, ascites, jaundice, asterixis, hepatic stench, gynecomastia, hepatomegaly, palmar erythema, testicular atrophy, gynecoid hair, and encephalopathy13-15.
Acute liver failure was considered when the duration of the disease was less than 26 weeks of evolution and without previously known liver disease10,11.
Patients were recruited from the gastroenterology department and evaluated for severity according to the Child-Pugh classification12.
Platelet/spleen indices lower than or equal to 909 were found to be normal1,6.
Hematic cytometry, liver function tests (in those older than one month from the previous control), upper gastrointestinal endoscopy with Fujinon endoscope model Eve EG 450WR5 and splenic ultrasound with Siemens Acuson X300 ultrasound were performed to determine the largest diameter of the spleen. For the statistical analysis, 2 x 2 tables were used for sensitivity, specificity, predictive values and test efficacy. Correlation of severity scales was performed with Spearman's rank correlation coefficient and a value of p≤0.05 was considered statistically significant. The study was approved by the Comité Local de Investigación y Ética en Investigación en Salud 2102 with registration number: R-2016-2102-12, and the anonymity of the participating patients was preserved at all times.
Findings
Seventy patients were recruited. The sample was predominantly male and geriatric patients. The characteristics in terms of sex, age and etiology of liver disease are shown inTable 1.
The average age was 59.58, minimum 35, maximum 85, SD=10.92 years. Regarding age groups, 3 (4.3%) patients were in the 18 to 40 years old group, 28 (40%) in the 41 to 60 years old group and 39 (55.7%) patients in the group older than or equal to 61 years old.
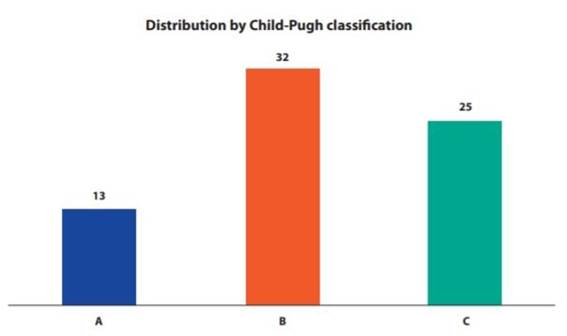
Regarding Child-Pugh classification, stage B was the most frequent with 32 (45.7%) patients. Details are shown in Figure 1.
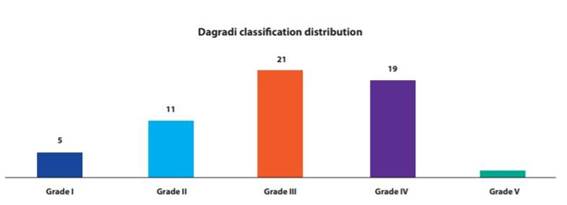
According to the Dagradi classification for esophageal varices(3), there were 21 (30%) Grade III patients. The rest of the details can be seen in Figure 2.
The correlation between P/B and Child-Pugh was 0.723, p<0.05, and between P/B and Dagradi was 0.585 (p<0.05), (a value of p<0.05 Spearman was considered statistically significant).
Of the 70 patients included in the sample, 47 (67%) patients presented esophageal varices at endoscopy and positive P/B index, 5 (7%) presented positive endoscopy for esophageal varices and 1.4% of patients presented negative P/B, with the following results: sensitivity 90%, specificity 83%, false positives 16%, false negatives 9%, positive predictive value of 94%, a negative predictive value of 75%, prevalence of 74% and a diagnostic certainty of 88% for P/B as a predictor of esophageal varices with risk of bleeding (Table 2).
Table 1. Population characteristics.
| Sex Etiology | Men | Women |
|---|---|---|
| Virus hepatitis C | 0 | 20 |
| Virus hepatitis B | 0 | 1 |
| Etilism | 31 | 0 |
| Unidentified | 11 | 7 |
| Total | 42 | 28 |
| Total of patients=70 |
Table 2. Comparison of the P/B index with endoscopy results.
| Endoscopic result | TOTAL | |||||||
|---|---|---|---|---|---|---|---|---|
| + | - | |||||||
| Índice P/B <909 | + | 47 | 3 | 50 | ||||
| - | 5 | 15 | 20 | |||||
| TOTAL | 52 | 18 | 70 | |||||
SENSIBILITY = a/(a+c) = 0,90 (90%).
FALSE POSITIVES = b/(b+d)=0,16 (16%).
POSITIVE PREDICTIVE VALUE = a/(a+b)=0,94 (94%).
PREVALENCE = (a+c)/(a+b+c+d) = 0,74 (74%).
SPECIFICITY = d/(b+d) = 0,83 (83%).
FALSE NEGATIVES = c/(a+c) =0,09 (9%).
NEGATIVE PREDICTIVE VALUE = d/(c+d) =0,75 (75%).
DIAGNÓSTICA CERTAINTY = (a+d)/(a+b+c+d) = 0,88 (88%).
AbreviatIons: + = positive, - = negative, P/B = platelets/spleen.
DISCUSSION
Portal hypertension is the main complication of chronic liver diseases that develop cirrhosis. It can cause esophageal varices in up to 30% of patients1,6-9,12. The most frequent causes are viral, alcoholic and of unidentified cause1.
Endoscopy is the diagnostic method of choice in HDA, it has high sensitivity and specificity since it records and identifies the location of the lesions that cause bleeding in the esophagus, stomach and duodenum. Nowadays, it is still the most accurate technique for diagnosing and staging esophageal varices, especially those of grade I, and for visualizing signs of risk for hemorrhage. This method provides the diagnosis and offers the possibility of a therapeutic approach4,5,13.
The frequency of bleeding esophageal varices is 100 in every 100,000 persons per year; it is a medical emergency associated with high mortality, especially in older adults1-3,5-9.
Esophageal varices, which occur in 100 out of every 100,000 persons per year, are a medical emergency associated with high mortality, especially in older adults1-3,5-9,13,14.
However, since endoscopy is an invasive diagnostic method, it has both relative and absolute contraindications. In developing countries, the availability of an endoscopic study is limited, therefore, different less invasive methods such as the P/B index have been implemented4,6-9,13,14.
The P/B index is inexpensive, is run quickly and requires no major skills for its performance. It is seen as a safe alternative in countries with limited economic resources that do not have endoscopy services, and another advantage is that it can be calculated rapidly6,8,13-15.
Since 2003, the high value of P/B has been demonstrated, even in the subgroup of patients with compensated liver disease6.
The value of P/B 909 or lower has been considered an indicator of esophageal varices(6,8,14,15). Reports in the Latin American population range from acceptable to very good for sensitivity, specificity and positive and negative predictive values8,14,15. In this study the results of the test in comparison with endoscopy were very high in sensitivity (90%), specificity (83%) and positive predictive value (94%), but low in negative predictive value (75%).
Some studies carried out in the Mexican population report a moderate correlation between P/B and esophageal varices: a P/B value greater than 0.7 correlated with Baveno grade I varices (<5 mm), and less than 0.7 with grade II varices (>5 mm) and with a low predominance in the advanced stages of Child-Pugh (of liver function) and Dagradi (of esophageal varices)14.
In this study, in which 70 patients were included, there was a higher correlation between P/B and Dagradi, with a higher percentage of patients in Child-Pugh stages B and C, compared to other studies.
As mentioned above, performing endoscopy for esophageal varices screening every one to two years in high-risk patients can be difficult and impractical9. Non-invasive parameters associated with high-risk esophageal varices help to reduce the need for endoscopic studies to be performed at this frequency and can be used to distinguish between high- and low-risk patients. This could be used to follow up only high- or very high-risk patients with endoscopic studies6,9,10,12.
It is also necessary to mention that a diagnostic endoscopy for esophageal varices should be performed in patients with risk factors, such as a Child-Pugh A12,13,15.
However, the P/B index is useful for stratification of cirrhosis patients into risk categories where portal hypertension data exist. This is especially relevant for those patients whose health status and conditions do not allow an invasive study, but who are at high risk of developing esophageal varices6,9,10,12.
In this study, most of the patients had Child-Pugh B and C classification. These stages are those with the highest risk to be associated with esophageal varices and bleeding according to international literature9,12-15.
The results of the test performed on the P/B index are consistent with other studies, although some show wide ranges of variability among them6,8,13-15.
The P/B is strongly associated with the presence of esophageal varices1,6,13,14, and its negative predictive value is reproducible, in this study with 75% and with a diagnostic certainty of 88%.
CONCLUSION
In conclusion, the P/B index presents false negatives of 9%, with a positive predictive value of 94%, a negative predictive value of 75%, with a prevalence of 74% and a diagnostic certainty of 88%, so it can be considered a useful and non-invasive study to diagnose esophageal varices especially in places, without availability of endoscopy.
REFERENCES
1. Narváez-Rivera RM, Cortez-Hernández CA, González-González JA, Tamayo-de la Cuesta JL, Zamarripa-Dorsey F, Torre-Delgadillo A, et al. Consenso Mexicano de Hipertensión Portal. Revista de Gastroenterología de México 2013; 78: 92-113. DOI: https://doi.org/10.1016/j.rgmx.2013.01.006 [ Links ]
2. Sverdén E, R Markar SR, Agreus L, Lagergren J. Acute upper gastrointestinal bleeding. 2018 Oct 25;363:k4023. DOI: 10.1136/bmj.k4023. [ Links ]
3. LaBrecque D, Khan AG, Sarin SK, Le Mair AW. WGO Practice Guidelines. Esophageal Varices. World Gastroenterol Organ Glob Guidel 2014: 1-14. Disponible en: https://www.spg.pt/wp-content/uploads/2015/11/2014-ESOPHAGEAL-VARICES.pdf. Consultado el 25/01/2021 [ Links ]
4. Jiménez-Rosales R, Valverde-López F, Martínez-Cara JG. Utilidad de Hemospray en hemorragia digestiva alta: análisis de los resultados en nuestro centro. RAPD ONLINE. 2018; 41: 8-13. Disponible en: https://www.sapd.es/revista/2018/41/1/01 [ Links ]
5. Pérez-Artimez M, Ferández-Duharte J, Brice-Abreu V, Dinza-Cabreja SA, Colas-Prevos GM. Ligadura de varices esofágicas por videoendoscopia en pacientes con hemorragia digestiva alta. MEDISAN 2020;24(6):1102. Disponible en: http://www.medisan.sld.cu/index.php/san/article/view/3413/html [ Links ]
6. Giannini E, Botta F, Borro P, Risso D, Romagnoli P, Fasoli A, et al. Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis. Gut. 2003; 52:1200-1205. DOI: 10.1136/gut.52.8.1200 [ Links ]
7. Giuffre M, Macor D, Masutti F, Abazia C, Tine F, Bedogni G, et al. Spleen Stiffness Probability Index (SSPI): A simple and accurate method to detect esophageal varices in patients with compensated liver cirrhosis. Annals of Hepatology 19. 2020; 53-61. DOI: 10.1016/j.aohep.2019.09.004 [ Links ]
8. Infante Velázquez Mirtha, Rosado Vargas Fer Coralia, Pérez Lorenzo Marlene, Samada Suárez Marcia, Hernández Amarán Mariela. Cociente conteo de plaquetas/diámetro bipolar del bazo menor que 909 para predecir várices esofágicas. Rev Cub Med Mil (Internet). 2013 Dic (citado 2021 Feb 03) ; 42( 4 ): 451-456. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0138-65572013000400005&lng=es. [ Links ]
9. Diagnóstico y tratamiento de várices esofágicas en el adulto. Guía de Evidencias y Recomendaciones: Guía de Práctica Clínica. México, CENETEC;(Intenert) 2017 (Citado el 25 de Enero 2021). Disponible en: http://www.cenetec-difusion.com/CMGPC/IMSS-087-08/ER.pdf. [ Links ]
10. Wendon J, Cordoba J, Dhawan A, Stolze-Larsen F, Manns M, Nevens F, et al. EASL Clinical practical guidelines on the management of acute (fulminant) liver failure. Journal Hepatol 2017; 66: 1047-1081. DOI: doi: 10.1016/j.jhep.2016.12.003. [ Links ]
11. Castro L, Nazal L, Silva G, Brahm J, Segovia R, Ferrario M, et al. Manejo de la falla hepática fulminante: propuesta de protocolo en Clínica Las Condes. Rev Med Clin Condes 2019; 30(2): 191-205. DOI: 10.1016/j.rmclc.2019.03.003 [ Links ]
12. Guía de práctica clínica Diagnóstico y tratamiento de la insuficiencia hepática crónica. México; Secretaría de Salud (Internet) 2009 (Citado el 21 de Enero 2018). Disponible en: http://www.cenetec-difusion.com/CMGPC/IMSS-038-08/ER.pdf. [ Links ]
13. Gralnek IM, Dumonceau JM, Kuipers E J, Lanas A, Sanders D S, Kurien M et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015; 47: a1- a46. DOI: 10.1055/s-0034-1393172 [ Links ]
14. Ramírez-Del Pilar R, Yáñez-Montes MC, Enríquez-Peregrino KG, García-Arias MR, Hernández-Mendiola R, López-González DS et al . Correlación del índice plaqueta/ bazo con el grado de várices esofágicas. Med. interna Méx. (revista en la Internet). 2017 Jun (citado 2021 Feb 03) ; 33( 3 ): 344-350. Disponible en: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0186-48662017000300344&lng=es. [ Links ]
15. Colli A, Gana JC, Yap J, Adams-Webber T, Rashkovan N, Ling SC, et al. Platelet count, spleen length and platelet count- to spleen length ratio for the diagnosis of oesophageal varices in people with chronic liver disease por portal vein thrombosis. Cochrane Database os Systematic Reviews 2017; Issue 4: Art. No.: CD008759. DOI: 10.1002/14651858.CD008759.pub2. [ Links ]
Received: January 16, 2021; Accepted: February 20, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
