










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.3 Lima jul./set. 2021
http://dx.doi.org/10.25176/rfmh.v21i3.3826
Original article
Risk of infections, chronic diseases and mental health disorders after floods by the coastal child phenomenon in displaced populations, Piura, 2017.
1Instituto de Investigación en Ciencias Biomédicas (INICIB), Universidad Ricardo Palma, Lima-Peru.
2Centro Nacional de Epidemiología, Prevención y Control de enfermedades.
2Director General del INICIB, URP, Lima-Peru.
Introduction:
In Peru, the presence of the Coastal Child Phenomenon produces floods and the appearance of diseases cyclically.
Objective:
To determine the risk factors for the presence of diseases in displaced populations in Piura due to the Coastal Child.
Methods:
Quantitative, longitudinal, analytical investigation of cases and controls with 544 families that were selected through a two-stage random sampling considering the proportion of families per block, area and cluster. For data collection, various diagnostic and monitoring instruments were used, such as that of the International Organization for Migration (IOM), the health care base and the application of an instrument for mental health.
Results:
The analysis of the variation of care in two time periods at 3 and 9 months shows that there are statistically significant changes in these periods that include skin infections, urinary tract infection, joint pain, diabetes mellitus and family violence. 26.46% presented some psychological disorder associated with coexistence in shelters. The bivariate analysis showed that families with less than 80% of safe water management and safe water storage were at risk of presenting acute diarrheal diseases with OR = 6.15 (95% CI 5.97-6.95) and OR = 2.08 (95% CI 1.06- 2.97) respectively.
Conclusion:
The epidemiological profiles show the presence of psychological effects and the transition of communicable diseases at the beginning of the disaster and that over time, non-communicable diseases and violence appear in the shelters associated with the previous health profiles of the displaced population.
Keywords: infectious diseases; non-infectious diseases; shelters. (Source: MESH - NLM)
INTRODUCTION
During the months of January and February of 2017, a climatologic event was presented in Peru that incremented the presence of rains, flooding and mud slides causing massive material damage that obligated the country to declare a state of emergency 12 departments. This phenomenon was called “The Coastal Child” that occurred due to the increment in superficial temperature of the Peruvian sea which intensified the continuous precipitations in the north coast of Peru. The city of Piura and several districts of this province were affected by floods that originated the collapse of safe drinking water systems and sewage systems, leaving miles of people affected that were displaced to temporary shelters.
Taking into consideration the prior epidemiologic profile of the affected area, the floods exacerbated the increase of infections with a potentially high epidemic risk in the population, such as vector-borne diseases, dermic diseases, and an increase in diarrhea illnesses. Likewise, the bad habits of water storage, inadequate sanitation conditions, lack of access to safe water and lack of sanitary installation obligated people to recur to defecating in the open air associated to a system of solid residue causing trash accumulation, increasing the risk of plagues and vectors in the temporary shelters.
The objective of the study was to determine the risk factors in the presence of diseases after floods due to the Coastal Child Phenomenon in displaced populations in Piura during the year 2017. Considering the epidemiological profile of the affected area, the floods exacerbate the increase of infection with high epidemic potential to the population as well as vector-borne diseases, dermic diseases, and an increase in diarrheal diseases. Likewise, safe water management and safe water storage were at risk of presenting acute diarrheal diseases the poor water storage habits, inadequate sanitation conditions, lack of access to safe clean water and lack of sanitary facilities force people to resort to defecating in the open air, associated with a management system of solid waste causing trash buildup, increasing the risk of plagues and vectors in the temporary shelters.
The objective of this study was to determine the risk factors in the presence of diseases following the floods from the Coastal Child Phenomenon in displaced populations in Piura during the year 2017.
METHODS
Design A quantitative, longitudinal, analytic case-control study was performed.
Population
The population consisted of families that were displaced in shelters created after the floods in Piura in March 2017 affecting populations of Castilla, Catacaos, Cura Mori, Narihualá and Simbilá. The grouping of the shelters took place in two clusters: one group located in kilometer 975 and the other located in kilometer 980 of the North Pan-American highway. These shelters are located 40 minutes from the city of Piura.
The first shelter cluster in kilometer 975 was organized in 5 areas: San José, Ciudad de Dios, Nuevo Buenos Aires, Nuevo Pedregal, Nuevo San Pedro and the cluster in kilometer 980 was organized in 7 areas: Cristo viene, Tupac Amaru I, San Martin, Santa Rosa, Eleuterio Cisneros, Jesús de Nazareth and Tupac Amaru II.
Each one of these areas were distributed by blocks and lots, which were assigned to the people registered as suffering by the affected areas. This area is characterized as being a deserted area without any basic service of water, sewage or electric power.
The family was determined as a unit of measure located in each shelter area for sample selection. A sketch of each location was set with the purpose of identifying the blocks and the locations of certain points such as water, hygienic services, trash pick-up, community centers, among others. The total number of families in the shelters was 2277. The sample size was 230 families for those sheltered in the kilometer 975 cluster and 314 families for those sheltered in the kilometer 980 cluster. For the selection of families, a two-stage random sampling was performed taking into consideration the proportion of families per block, area and cluster.
The inclusion criteria were to have a family member or other person of both genders, over 15 years of age, that were present during the interview and that the family who resides in the shelter areas has a minimum of 3 months residing in the area.
Procedures
For the information collection diverse collection instruments were used. One of them was the secondary base of information taken to the shelters by the Organización Internacional para las Migraciones (OIM), where the inhabitants were asked various questions regarding housing, diet and nutrition, education, measures of livelihood, security, dignity and privacy and communication and community participation. We also used the sheltered people’s health records from the mobile health centers distributed in both shelter clusters. Likewise, a general health questionnaire (GHQ-12) which has proven to be an effective tool for mental health assessment in the general population and the clinic population. This questionnaire was created for the purpose of identifying two types of problems: the incapacity to perform daily normal or adaptive activities and the manifestation of disruptive phenomenon and the subject’s psychopathologic symptoms. This questionnaire includes 12 Likert-type items that explore mental health symptoms during the last month, with an ordinal type of response made up of four answers from never to always.
Statistical analysis
The data collected from the information sheets was entered into Excel spreadsheets after quality control and verification of information from tracer illnesses of the epidemiologic surveillance system of DIRESA Piura. We used the information from the data bases provided by the OIM and from international cooperators such as the Italian International Cooperation (COOPI) who was in charge of the project of safe water, sanitation and hygiene improvement provision for the people affected by the floods and displaced to shelters in Piura and Morropon.
Various descriptive analyses of the diverse variables were performed and compared in time to see the disease progression at 3 and 9 months. Likewise, an inferential analysis was performed, and the analytical statistic will be applied with a confidence interval of 95% (CI95%) and a significant p-value of p<0.05 as statistically significant.
Ethical considerations
The anonymity of personal data was taken into account for the development of the study according to Law N° 29733 (“Law of Protection of Personal Data”), both for the database used as for the collection of epidemiological information. Likewise, a participant informed consent was requested to undertake the survey. The Project was approved by the Research Ethics Committee of the Universidad Ricardo Palma.
RESULTS
Population characteristics
The sample was comprised of 544 families from two shelter clusters in Cura Morí. From the total number of families, we were able to compile information from 616 people who lived in shelters for more than 3 consecutive months. Of 32.3% (199/616) were of masculine gender and 67.7% (417/616) were of the feminine gender. This phenomenon was due to the majority of men working in locations where they lived prior to the floods and were restoring the land for agriculture. Likewise, in age groups we can observe men between 21 and 40 years of age represented 44.7% (89/199) of the total men, while women were close to 50% (201/417). This connotation in the grouping of men and women was observed in the organization of shelter areas, and that women were dedicated to the feeding of the sheltered and the men in the security tasks and wellbeing of the inhabitants. The family distribution by areas in each cluster was different. In the cluster formed in kilometer 975, the areas of Ciudad de Dios, San Pedro and Nuevo Buenos Aires represent 84.33% of the sheltered in this cluster. While those sheltered in kilometer 980, 66.35% were concentrated in the areas of de Cristo Viene, Jesús de Nazareth and Tupac Amaru I.
Epidemiology of tracer illnesses
Three months after initiating the displaced inhabitant’s residence in the shelter areas, a total of 1236 medical services were registered in the mobile health posts from the Ministry of Heath. Of these, 37% were registered for lesions of external causes, which include lesions, bruising, puncture wounds in various parts of the body. The second cause for medical attention were acute respiratory infections with 17.9% comprising pharyngitis, rhinopharyngitis, acute tonsillitis, otitis media. It is important to consider that bronchopneumonia and severe pneumonia cases were not registered in the shelter population. As third cause with 10.5% were skeletal muscular pain which included arthralgia, back pain, and low-back pain. The fourth cause were psychological disorders with 5.6% comprising states of anxiety and depression due to the loss of their belongings, property, family and start all over in a place of difficult access. The fifth cause had 5.5% were the acute diarrheic diseases which, despite not having safe drinking water and sewage, safe water supplies and chemical baths were implemented in various points which controlled the dissemination of diarrheic diseases.
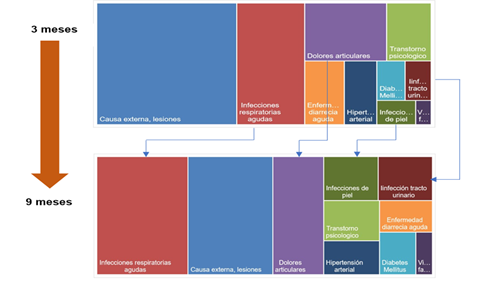
Figura 1. Polygon graphic, comparison from tracer illnesses of epidemiological vigilance at 3 and 9 months in shelters in Piura 2017.
At 9 months of living in shelters, the total visits were 3619 notes, which means they tripled in 6 months. However, it is obvious that the reasons for medical care changed. The first cause for this evaluation period was respiratory infections which represented 21%, followed by the lesions of external cause with 20%. In this period the following appeared as reasons for medical attention, in order of importance, skin diseases in 4.7% which included dermatitis, impetigo, tinea corporis, pyoderma, urinary tract infection and hypotension with 3.8%, the most affected group were those above 60 years of age which represented 67% for this medical attention.
Changes in the tracer illnesses profile
Upon comparing the causes for medical attention in the two time periods of 3 and 9 months, we observe that the causes changed. Respiratory infections moved to first place after finalizing the assessment. It is obvious that in the polygon graph we observe an increase in diseases associated to joint pain where they tripled compared to the initial period, associated more to medical attention for arthrosis, lower back pain and upper back pain.
Another important change was that skin disease increased in this assessment period. They increased six times more than the initial period, and it was associated to skin infections, acariosis and tinea corporis.
We observed that causes for medical attention associated to non-transmissible disease increased, such as hypertension and diabetes mellitus, almost 3 times and medical attention for family violence increased by 5 times.
In the analysis of variation of medical attention in two time periods at 3 and 9 months we observe that there are statistically significant changes in these periods that include skin infections, urinary tract infections, joint pain, diabetes mellitus and family violence. An important analysis is how tracer illnesses associated to external causes and acute diarrheic diseases decrease significantly in these two time periods.
Table 1. Tracer illnesses from epidemiologic vigilance at 9 months of permanence in shelters. Piura 2017.
| Daños trazadores | 3 months | 9 months | Brecha | p |
|---|---|---|---|---|
| Infecciones respiratorias agudas | 18.0 | 21,6 | 3,59 | 0,06 |
| Skin infections | 2,0 | 4,8 | 2,76 | 0,001* |
| Infección tracto urinario | 2,3 | 4,8 | 2,49 | 0,003* |
| Dolores articulares | 10,4 | 12,0 | 1,66 | 0,04* |
| Diabetes Mellitus | 2,4 | 3,1 | 0,67 | 0,05* |
| Violencia familiar | 0,8 | 1,4 | 0,57 | 0,05* |
| Hipertensión arterial | 4,5 | 3,8 | -0,72 | 0,07 |
| Transtorno psicológico | 5,7 | 4,5 | -1,16 | 0,06 |
| Enfermedad diarréica aguda | 5,5 | 3,3 | -2,16 | 0,001* |
| Causa externa, lesiones | 37,1 | 20,0 | -17,02 | 0,002* |
*p<0,05
Psychological disorders in people in shelters
According to the results of the application of mental health scale GHQ12, we found from the total of 616 interviewed, 26.46% (163/616) had some kind of psychological disorder associated to the cohabitating in shelter areas and are exposed to various factors and stress conditions in the housing area.
Out of all patients, 2% (12/616) had a disorder, such as anxiety detected, and which had greater depression traits during the interviews. 3% (18/616) had a depression type disorder detected, associated to deep sadness, insecurity, and loss of interest in what they do.

Considering that the people in shelters were distributed in two clusters, the analysis was done per zone. Among those sheltered in kilometer 975 of the Pan-American North highway, 37.4% (86/230) presented with a psychological disorder, Ciudad de Dios presented the greatest number of cases in this area with 37.2% (32/86), followed by Nuevo San Pedro with 24.4% (21/86). Upon performing the analysis of those sheltered in kilometer 980, in the area of Cristo Viene there were 29.1% (35/120) of the total number of psychological disorder cases, followed by the area of Jesus de Nazareth which presented with 21.6% (36/120) of those sheltered with this disorder.
Water
They lack safe drinking water; they are supplied with water tanks that deposit water in tanks of 500 liters or buckets installed at various points in the shelters. The water tanker truck provides water from a distant area and according to the OPS/OMS team information, the water source was evaluated, and it was reported that it lacked chlorine. Due to the difficulty of the sandy soil, the water tankers deposit water closes to the highway trail and the people have to go there with buckets to take water back to their homes.
Storage is through tanks provided by INDECI and other organizations, however, not all of them are closed adequately in order not to allow insects or other particles inside. We were with the OPS/OMS commission verifying the quality of water through the measure of chlorine and observed that the deposits do not have enough residual chlorine in their storage, which is why a campaign was started for the measure of chlorine in these containers by the health resources in these service stations.
Electric Flow
Some of the groups have a generator that works with a solar panel and they use it from 6 to 10om. They also have aerial speakers and a communication cabin that allows them to send massive messages to these populations.
Sewage
We observed various chemical baths installed by the businesses in both shelters. Cleaning is performed every 2 to 3 days, However, those chemical baths installed far from the highway have a cleaning every 6 to 7 days due to the difficulty in geographic access. It is impossible to have a cesspit due to the sandy soil, which is why there are several inhabitants who have to relieve themselves in the open terrain.
Food
With respect to food, it is done in community kitchens where the mother’s group together to make breakfast, lunch and dinner Monday to Saturday. The food is prepared based on donations given by INDECI and other contributors. The products that are given include pasta, oil, tuna, rice among others. If some of the groups decide to include chicken or meat, they must have an additional collection to buy these food items.
The kitchens are mostly open which is why they are exposed to permanent contamination. Also, they use wood as fuel consumption to prepare the food.
Table 2. Risk factors associated to the presence of disease in people sheltered due to the floods of the Coastal Child Phenomenon. Piura 2017.
| Risk Factors | Indicator | Acute Diarrheic Disease | OR | P | Acute Respiratory Infection | OR | P | Skin Diseases | OR | P | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sí | No | Sí | No | Sí | No | ||||||||
| Food reception | <80% familias damnificadas que reciben ración alimentos | 35 | 86 | 2,29 (0,89-3,46) | 0,3141 | 68 | 17 | 1,61 (0,89-1,98) | 0,231 | 28 | 29 | 1,15 (0,85-1,39) | 0,210 |
| Manejo de agua segura | <80% familias damnificadas que tienen agua segura | 34 | 125 | 6,15 (5,97-6,95) | 0,000 | 82 | 44 | 2,62 (0,99-1,99) | 0,089 | 52 | 32 | 2,38 (1,08-3,97) | 0,065 |
| Almacenamiento de agua | <80% familias damnificadas con recipientes de agua segura | 23 | 98 | 2,08 (1,06-2,97) | 0,004 | 74 | 22 | 2,46 (1,98-3,01) | 0,328 | 68 | 22 | 2,01 (1,08-3,56) | 0,214 |
| Eliminación de residuos sólidos | <80% familias damnificadas con envases para recolección residuos sólidos | 103 | 18 | 1,31 (0,75-1,73) | 0,015 | 85 | 25 | 2,62 (2,04-3,04) | 0,084 | 42 | 75 | 3,27 (3,02-3,86) | 0,010 |
| Distribution of hygiene inputs | <80% familias damnificadas con kits de higiene | 92 | 28 | 1,01 (0,23-1,63) | 0,089 | 38 | 117 | 4,26 (3,98-4,62) | 0,000 | 28 | 120 | 5,26 (4,92-5,93) | 0,000 |
| Acciones y cuidado personal | <80% familias damnificadas que participaron en charlas preventivas | 82 | 54 | 2,56 (1,56-3,01) | 0,256 | 56 | 64 | 1,89 (1,18-2,14) | 0,005 | 31 | 98 | 4,22 (3,91-4,74) | 0,030 |
Solid waste collection
Solid waste has various treatments in some shelters. They have been given bags and they accumulate for their later collection by the municipal truck which passes by every 3 to 4 days. Others burn the waste and bury them in an open field. There is no solid waste segregation.
In the shelters located in kilometer 98 they practice more burying the waste in an open field since the municipal truck cannot reach these shelters due to the difficult terrain access.
Quick evaluation of environmental determinants in community kitchens
During the visit to the camp, an interview was conducted to the mothers of the community kitchens and they were asked about the environmental risk factors. 6 kitchens were evaluated: Pedregal Nuevo, San José, Túpac Amaru I, Túpac Amaru II, Cristo Viene. All had in common that they used Wood as fuel consumption for cooking the meals, they are in open fields, water consumption is provided by a cystern water tank, which does not count with adequate chlorine. Food prepared are mostly carbohydrates donated by INDECI and other organizations.
Solid waste in places near the Pan-American entrances are picked up by the municipal garbage truck every 3 to 4 days, while far away shelters burn and bury the solid waste in open fields.
Evaluation of risk factors in people living in shelters after floods in Piura
According to the description in determining factors associated with the presence of diseases, it has been determined that six factors could be contributing to the presence of disease in these clusters.
These factors are food reception, safe water management, water storage, solid waste removal, hygiene product distribution and hygiene practice and personal care. All of these factors were Split into two groups: those with indicators of 80% or more and the group with <80% of affected coverage and the presence of trace illness was determined.
From the analysis, we observed that the presence of acute diarrheic diseases was present where there were less than 80% of affected families with safe water and less than 80% with water storage in containers, with OR= 6,15 (5,97-6,95) CI95% y 0R= 2,08 (1,06-2,97) CI95%, respectively.
Acute respiratory disease was present where there was less than 80% of affected families with hygiene kits and preventive talk participation, with an OR=4,26 (3,98-4,62) CI95% y 0R= 1,89 (1,18-2,14) CI95%, respectively. Skin diseases were present where there was less than 80% of affected families with hygiene kits, with an OR=5,26 (4,92-5,93) CI95%.
DISCUSSION
Despite that the appearance of an infectious process after a disaster is one of the most rooted ideas, not only among the people and media, but also among the healthcare workers, what is true is that communicable disease outbreaks appear in very specific types of disasters (for example in floods that modify the ecosystems of certain vectors such as Aedes or Anopheles mosquitoes or in poor hygiene and health conditions of people living in these shelters.8
The epidemiological watch of trace illnesses allowed to identify the need for attention of the displaced population. However, it is necessary to determine the risk factors associated to water management and collection, basic sanitation and security in the shelter, that allows us to mitigate the presence of epidemic outbreaks.
Safe water availability
The presence of diarrheic disease was 6.15 times more than those shelters where families had less than 80% safe water and it coincides with what Arcos P.8mentioned which affirms that unsafe water is one of the main problems of communicable diseases among the displaced populations. The value of this criteria includes the water storage condition determined for the availability of water storage per person. It was found that the mean reaches 19.6 liters, in the same manner the supply capacity measured by the real availability of water by people.
The value of this criteria includes the water storage condition determined by the availability of water storage by the person. It was found that the mean reaches 19.6 liters, in the same way the storage capacity is measured by the real water availability by people, and it was found this was 18 liters. Another one of the conditions that include the criteria is referred to water sufficiency which was measured by the activities that allow them to supply the water they have. In this manner it was found that 65% of families refer having enough water to drink and cook, 51% of them have enough water to drink, cook and perform personal hygiene. Only 40% of families surveyed reported having enough water to drink, cook, for personal hygiene and washing. The shelters that reported having greater water availability were San Martin and Jesus de Nazaret.
An important aspect is also the distance between housing and the point where the water is located. We found that on average it was 55 meters away, however, we observed areas where the distance reaches 200 meters. In the shelter Tupac Amaru II the average distance reached 70 meters.
In relation to storage quality, two conditions were evaluated: keeping the storage units covered and that they be washed by brush at least once a week.
Regarding this, we found that the average of covered storage containers was 96% and 94% brushed these storage containers. The last condition that evaluates this criterion is related to treating water that is consumed, with respect to this, it was found that 100% of families consume treated water. 86.7% consumes it by boiling water, 10.8% reports that they chlorinate it and 2.5% filters the water. The final result of this criteria reached a value of 62.5%. The most important preventive measure for infections associated to water was the use of safe water for drinking and washing food (fruits and vegetables) as it was referred by Moran F and Ochoa T.10The recommendation, in order of, is use bottled water, in second place boiled water and in the case of cloudy water, it may be filtered through a cloth or let it sit and take the clear water out. In third place, you may use chlorinated water. Disinfectants, such as chlorine/bleach may kill the majority of viruses and bacteria that cause diseases, but they are not as effective in the control of the most resistant germs, such as the Cryptosporidium y Giardia parasites.(11)
Hygiene practices
The shelters with less than 80% of hygiene kits presented 1.01 times more diarrheic diseases and 5.26 times more skin diseases. Likewise, despite that the actions and personal hygiene were not significant in the research, they were for Moran F and Ochoa T10to consider them for the presence of diseases. This criterion incorporates five conditions. The first is the access to hand washing which was assessed as the number of times family members washed their hands in one day. It was found that in the majority of families (67%) reported washing their hands 4 or more times and 30% reported washing their hands two to three times a day. The assessment of the moment in which handwashing occurs were reported to be before eating (83%), before cooking (76%), and after leaving the bathroom or latrine (73%).
The criteria also evaluate handwashing condition whether it is only with water or with water and soap. The majority of families reported washing hands with soap and water (91%). Another one of the conditions is if families have soap for personal use. It was found that 94% count on having soap. This information from the field research by the Italian Cooperation Agency, are similar to those found in this study.
Access to decent and safe latrines
The assessment of the accessibility condition considered the presence of latrines and/or chemical baths in the shelter population. It was found that 54/2% of the population reported using latrines installed by the projects (mainly in the shelters Tupac Amaru I and II) and 41.7% make use of the chemical baths installed by the government. However, 4.2% use open fields to relieve themselves (mainly in shelters San Rosa and Jesus de Nazaret), an important factor in the presence of communicable diseases as mentioned in the epidemiologic vigilance manual from the OPS3. Regarding the distance to the latrine and/or chemical bath, from the housing point, it was found that 60% reported that they are less than 50 meters away. The shelter population of Jesus de Nazaret reported a far distance from the latrine/chemical baths. The analysis regarding latrine/chemical bath privacy reached a high assessment by the inhabitants in all shelters (86%), same as the comfort condition which reached a score of 93.9%. The cleaning condition was assessed by the hygiene from the latrine and/or chemical bath, which the majority reported that it was every other day (59%) and daily (23.3%). The safety conditions for boys and girls were evaluated by the informant’s assessment to define and reach a value of 75%. On the other hand, the use of latrines/chemical baths by the disabled population was asked and we found that 94% of them sit comfortably while using them.
Good practice of solid waste disposal
According to the survey by COOPI 12, it was found that generally 39% of families surveyed reported storing them inside their home, while still and elevated proportion of families store them outside their home. The weakest points are in shelters of Jesus de Nazaret and Santa Rosa. In the same manner, it was found that the storage means that the inhabitants use with most frequency are bags (81%). On the other hand, the assessment of the final disposal of solid waste was found to be 51% done by the garbage trucks/motorcycles followed by 39% of families that use the “garbage cans” implemented by this project. However, there is still 10% that use other sources such as “open fields”, burying them or burning them to dispose of solid waste.
People with Access to safe human settlements
The exploration of identifying the protection path for abuse and violence cases reached an assessment of 47.5% in the survey done by COOPI, and for sexual child abuse and sexual violence it was found to be 34% of families that identified the protective path. Likewise, regarding the messages of family care, it was found that 56.7% of families remembered 2 or more messages related to the topic, of which stand out the most are show of affection with caresses, loving expressions and allowing girls, boys and adolescents participate in cultural, playful and recreational activities. With respect to the protection path that they should follow in case of violence and others, they identified in the first place the Red Cape (a red tent by the Women Ministry) installed in the shelter surroundings to receive and help people that had their rights violated. This information, complementary to the study, has allowed the health establishments to register cases of violence and, through these, the corresponding entities installed in the shelters can be notified.
CONCLUSION
In conclusion, the population displacement of people affected by disasters as the ones mentioned in the floods in Piura by the Coastal Child Phenomenon associated to the epidemiological health profiles in these affected areas, increase the potential risk of diarrheic diseases, skin infections, respiratory diseases and non-communicable disease and the control of the damages depend on post-disaster organization to mitigate the determinants which could generate epidemic outbreaks.
REFERENCES
1. Rodríguez A, Terry B. Guía práctica para la fase de emergencia en caso de desastres y poblaciones desplazadas. Rev Cubana Hig Epidemiol [Internet]. 2002 Ago [citado 2018 Ago 15] ; 40( 2 ): 112-120. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-30032002000200006&lng=es. [ Links ]
2. Terry B, Rodríguez A. Una estrategia de atención primaria de salud en situaciones de desastres. Gac Sanit [Internet]. 2005 Feb [citado 2018 Ago 15] ; 19( 1 ): 76-79. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-91112005000100015&lng=es. [ Links ]
3. Organización Panamericana de la Salud. Vigilancia epidemiológica sanitaria en situaciones de desastre: Guía para el nivel local. Programa de Preparativos para Situaciones de Emergencia y Socorro en Casos de Desastre. Serie Manuales y Guías sobre Desastres, N.º 2. Washington DC, Septiembre, 2002. [ Links ]
4. Maguiña C, Astuvilca J. Desastres naturales y prevención de enfermedades. Acta méd. Peru [Internet]. 2017 [citado 2018 Ago 22]; 34 (1):3-5. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1728-59172017000100001&lng=es. [ Links ]
5. Espinoza-Neyra C, Jara-Pereda M, Díaz-Vélez C. Trastorno de estrés postraumático en una población afectada por inundaciones ocasionadas por el niño costero en Perú. Rev. Perú. med. exp. Salud pública [Internet]. 2017 [cited 2018 Sep 03]; 34(4): 751-752. Available from: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1726-46342017000400025&lng=en. http://dx.doi.org/10.17843/rpmesp.2017.344.3058. [ Links ]
6. Morán F, Ochoa T. Prevención, diagnóstico y tratamiento de infecciones pediátricas en desastres naturales. Rev Peru Med Exp Salud Pública. 2017; 34 (4): 723 - 730. Disponible en: https://doi.org/10.17843/rpmesp.2017.344.2810 [ Links ]
7. Terry B, Rodríguez A, García M. Comportamiento de la morbimortalidad y manejo de riesgo en población afectada por un evento sísmico. Rev Cubana Hig Epidemiol [Internet]. 2006 [citado 2018 Ago 22] ; 44( 3 ). Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-30032006000300002&lng=es. [ Links ]
8. Arcos P, Castro R, Busto F del. Desastres y salud pública: Un abordaje desde el marco teórico de la epidemiología. Rev. Esp. Salud Pública [Internet]. 2002 [citado 2018 Ago 23] ; 76( 2 ): 121-132. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-5727200200200006&lng=es. [ Links ]
9. Saul P. Problemas de salud en desastres naturales. Medwave. 2010;10(10):e4794 DOI: 10.5867/medwave.2010.10.4794 Disponible en :https://www.medwave.cl/link.cgi/Medwave/Reuniones/4794 [ Links ]
10. Híjar G, Munayco C, Gutiérrez E, Ramos W. Fenómeno El Niño y Salud Pública. Rev Peru Med Exp Salud Publica. 2016;33(2):300-10. [ Links ]
11. Morán F, Ochoa T. Prevención, diagnóstico y tratamiento de infecciones pediátricas en desastres naturales. Rev. perú. med. exp. salud pública [Internet]. 2017 [citado 2019 Sep 16]; 34( 4 ): 723-730. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S172646342017000400021&lng=es. http://dx.doi.org/10.17843/rpmesp.2017.344.2810. [ Links ]
12. Línea de base final del proyecto de ayuda humanitaria en los sectores de WASH y PROTECCION a personas afectadas por las inundaciones en Piura - Perú. Cooperazione Internazionale. COOPI. Octubre 2017. [ Links ]
Received: March 16, 2021; Accepted: May 31, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
