










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.3 Lima jul./set. 2021
http://dx.doi.org/10.25176/rfmh.v21i3.4016
Review article
Damage control approach and reduced resuscitation of the polytraumatized pediatric patient in the emergency room
1Hospital Pediátrico Peralvillo SSCDMX, Ciudad de México México
2Hospital de Traumatología y Ortopedia, IMSS, Monterrey, N.L, México
Polytrauma in pediatric patients is a frequent event, so its timely approach and management define its prognosis. Polytrauma is defined as the presence of two or more traumatic injuries or a single one that endangers life or there is a risk of serious sequelae; resuscitation is understood as the restoration of vital functions of the patient in the pre-hospital area to the hospital area aimed at avoiding the damage caused by the fatal pentad of trauma (coagulopathy, acidosis, hypothermia, hyperglycemia and hypoxemia) for which the damage control protocol was carried out, which is referred as all the maneuvers that have the purpose of preserving life, but without carrying out definitive repairs in order to mitigate complications derived from the prolonged state of shock, secondary to a prolonged surgical time that postponed adequate resuscitation, this reduced resuscitation consists of 6 precise indications for its performance, being approached from the TEP (Pediatric Evaluation Triangle) and the MARCHDEF protocol (Massive Bleeding, Airway, Breathing, Circulation, Hypothermia, Neurological Deficit, Glycemia, Pain, Exposure, FAST).
Keywords: Polytrauma; Damage control; Reduced resuscitation; TEP; MARCHDEF (source: MeSH NLM).
INTRODUCTION
When a patient has two or more traumatic lesions or only one that puts their life in danger or at risk of undergoing serious sequelae, we define the concept of polytrauma, cranioencephalic traumatism as the most frequent and often associated to lesions in other parts of the body. Death in a pediatric patient with polytrauma generally occurs within the first minutes after an accident and the most frequent reported causes are lesions to the brain, medulla and major vessels. Only a third of deaths (30%) occur hours aft4er the accident due to hypovolemia, hemorrhage or hypoxia.
Immediate resuscitation
Resuscitation is the reestablishment of the child’s vital functions, in this case, trauma victim where pre-hospital care is begun to continue to hospital care with the necessary invasive procedures to diminish and avoid damage caused by coagulopathy, acidosis, hypothermia and hypoxia1. This concept was first applied during the Vietnam War where trauma lesions were observed that caused coagulopathy and acidosis, for which early hemotransfusion with reconstituted blood was proposed. During the Afghanistan War, in the first decade of the XXI century, patient care with high energy trauma was systematized and the damage control resuscitation or immediate resuscitation thinking was applied1. In the decade of 1970, the University of Pennsylvania proposed the damage control protocol that included the patient care with trauma of high energy, multiple fractures and state of exsanguinating shock, referred to all maneuvers that had the goal of preserving the patient’s life, without taking definitive repairs since they take time and perpetuate the state of shock and hypothermia in the patient. Patients died more from prolonged state of shock derived complications, secondary to prolonged surgical time that postponed the optimal patient resuscitation.
There are six resuscitation indications with damage control:
Lesion severity, defined by the presence of two lesions or organs or systems that place the patient’s life in danger, the majority of times they are secondary to high energy trauma or have damage severity index greater than 35 points.
State of exsanguinous shock with a loss of circulating volume in the pediatric patient (80 a 90cc kg) of 28% or more during more than 70 minutes, which could be complicated with consumption coagulopathy.
Invest time in procedures that don’t improve patient survival or the insufficient medical experience while conducting same.
Hypothermia less than 34°, acidosis with pH <7,2 and coagulopathy (prothrombin time >19sec, partial thromboplastin time <60 o >60 sec, serum lactate > 5 mmol/L and base deficit > 6mmol/L).
Failure to block external and internal hemorrhages (intrabdominal or thoracic).
Presence of associated comorbidities such as diabetes, obesity, cardiopathy, renal insufficiency, malformations, age below 5 years or greater than 60 years1.
Clinical approach
The recommended model for evaluation consists of a general and initial evaluation of the child through a pediatric evaluation triangle (TEP) and the first, second and third evaluations. The goal was to recognized signs of central nervous system dysfunction, respiratory insufficiency, compensated shock and decompensated shock to promptly intervene and save the patient’s life. If patients are not treated promptly, they can rapidly progress to cardiopulmonary insufficiency whose final outcome is cardiac arrest2.
The basic care outline is the following:
General evaluation
Primary evaluation (MARCHDF system)
M. Massive hemorrhages
Airway
R. Respiration
Circulation
H. Hypothermia
Neurologic deficit/Capillary glycemia (Destrotix®)/Neurologic incapacity (Glasgow), Pain
Exposure
F Drugs, FAST, Family.
Secondary Evaluation (MESIRT System)
General evaluation
Use the “evaluate-identify-intervene” model to evaluate and treat the pediatric patient who is hurt and critical. Performa an initial evaluation and proceed to repeat the evaluation in order to decide the best treatment and patient intervention. Categorize the clinical status according to the type and severity, decide and act to initiate treatment. Later, reevaluate and repeat the process “evaluate-identify-intervene”. If a potentially deadly inconvenience is identified, proceed to initiate the necessary interventions to sabe the child’s life and use the evaluation with a systematic approach1,2,3,4,5.
Pediatric Evaluation Triangle TEP
TEP is an approach for the initial evaluation, specially adapted for children, It is a quick, simple and useful tool to evaluate children of all ages. It allows the patient characteristics to be integrated with those of general impression independently from the illness or lesion. TEP has become the basic evaluation model in national and international programs of vital support1. It is a simple instrument to begin the evaluation of a child exclusively based on visual and auditory indices, not requiring a stethoscope, sphygmomanometer, cardiac monitor, or pulse oximeter. Use the TEP tool wherever the first patient is done, the evaluation should be done in 30 to 90 seconds. TEP is the evaluation paradigm at first sight. The three components of TEP reflect the general physiological state of oxygenation, ventilation, perfusion and cerebral function. The components of TEP are appearance (conscience or unconsciousness, irritability, hyperactivity, hyporeactivity, and bleeding), circulation (cyanosis, paleness, and marbled skin) and respiratory (apnea, dyspnea, polypnea or bradypnea). TEP is a tool and not an instrument that helps first contact health personnel offer support to the patient in an emergency situation. The three components in TEP (Figure 1) allows the initial evaluation of cardiopulmonary state, cerebral function and metabolism of the child, as well as identification of the type and severity of the physiologic state to initiate treatment as soon as possible1,2,6.
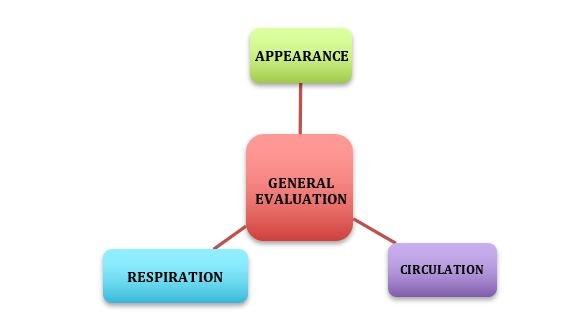
Figure 1: Concept of general evaluation or TEP: a.Appearance: Alteration of consciousness or bleeding. b.Circulation: Color, cyanosis, paleness, marbled, etc,. c.Respiratory: Increase or decrease of respiratory work or abnormal sounds such as stridor or respiratory sounds.
If the patient presents respiratory difficulty, they will be placed in a comfortable position and administer supplemental oxygen as required, furthermore the specific therapy for the possible etiologies is begun, If the patient presents respiratory insufficiency, the head position, airway permeability are reviewed and oxygen is administered at 100% through bag-mask ventilation as needed. If the patient has foreign bodies, we proceed to extract them. Lastly, we obtain an advanced airway.
Oxygen is administered for patients with shock.
In a vital risk situation, it is important to verify the adequate head position, maintain a permeable airway and if necessary proceed to orotracheal intubation, ventilation is initiated with the corresponding device, oxygen at 100% is administered and resuscitation maneuvers are initiated.
Due to TEP being easy and practical to perform and record, it ensures that all health personnel involved in the emergency services “speak the same language”, allowing to rapidly categorize the alteration that the pediatric patient presents. It constitutes the first step to prioritize critical patient care who comes to the emergency room by only responding to the following questions:
How serious is the pediatric patient’s lesion?
What is the probable physiological abnormality?
What is the urgency in the care to initiate treatment?
The three components are essential to improve efficiency and efficacy in care, both quality indicators in the emergency room.7.
Primary evaluation
The primary evaluation is the clinical evaluation that consists of a rapid and systematic exploration for the purpose of detecting lesions that constitute a vital risk to the patient. The treatment must be effective and simple.
MARCH-DEF System
An acronym used and accepted by the United States trauma committee for the management and approach of the ten platinum minutes in the pediatric patient and the polytraumatized adult in a conventional and hostile pre-hospital and hospital setting1,7,8.
M Massive hemorrhage
The first cause of death within the first hour of trauma care is exsanguinous bleeding that provoked hemorrhagic shock, acidosis, and consumption coagulopathy within a short time. The rapid, effective and efficient control of exsanguinous hemorrhage with compressive agents (turnstiles, compressive bandages, hemostatic gauzes, etc.) and hemostatic agents according to protocol, victim state and place of situation, is priority in polytraumatized patient care. A hemorrhage that compromises a main vessel, artery, or vein, may provoke death within five to ten minutes. Therefore, the hemorrhage management is of maximum priority9,10.
Systemic hemostatic agents
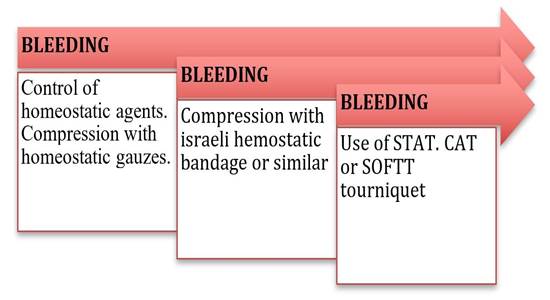
Tranexamic acid (ATX) is a synthetic derivative of the amino acid lysine and inhibits fibrinolysis through the blockage of lysine fixation sites in the plasminogen, which could be administered in a wide gamma of pathologies in the medical care environment. Children have a reduced blood volume compared to adults and cannot tolerate great losses of blood volume. However, the lack of cardiac and vascular diseases in them allows a greater compensation capacity during hemorrhagic shock10. The incidence for ATX use in pediatric trauma is low. However, we consider that its incorporation in the management of pediatric trauma has the potential to significantly reduce mortality in children and young people without increasing the adverse events, which is why it is suggested to consider its use. Its early application is recommended following protocol used in adults. The loading dose of 1g applied within 10 minutes during the first 3 hours after a lesion, followed by an infusion of 1 g during 8 hours for children over 12 years of age. For those under 12 years of age, the loading dose is 15mg/kg (maximum dose 1 g) followed by an infusion of 2mg/kg/hour during at least 8 hours or until bleeding stops. The adverse effects of TXA in pediatrics is rare, however, under the context of trauma we acknowledge that more research is necessary since some studies have very low levels and grades of recommendations. The first measure of care is direct compression with hemostatic gauze or Israeli compressive bandage10,11. (Figure 2).
Tourniquets
Few studies have been published in relation to the prehospital experience with tourniquets in children. The Pediatric Trauma Society supports the use of tourniquets in prehospital environment and during resuscitation in patients who suffer from exsanguinous hemorrhages (C/D recommendation grade) *. We must remember that during the Boston attack many victims were children and the first responders placed tourniquets to various pediatric victims with exsanguinous hemorrhages that saved lives with this simple intervention. In the year 2012, the TECC (Tactical Emergency Casualty Care) pediatric guide appeared in which its use is allowed in the pediatric patient. Children who are victims of violence generally present similar lesion patterns as adults. Therefore, in them the use of tourniquets may also be indicated with the aim in seeking hemorrhage control in their extremities. After the Boston attack, the American Academy of Pediatrics recommended the use of STAT type tourniquet in children. With the aim of obtaining maximum security and clinical use in pediatric patients from the different age groups, it is necessary to perform research in the pediatric field to evaluate the size of the tourniquets taking into consideration the child’s physiological characteristics and other aspects related with these types of patients.12.
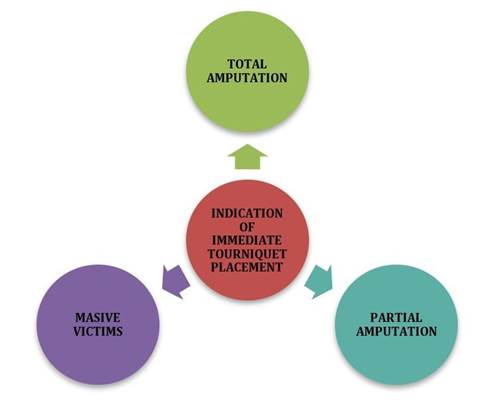
Absolute clinical indications for immediate tourniquet placement in pediatrics: (Figure 3)
In amputations of important magnitude with moderate or severe external hemorrhage.
Important bleeding not controlled by direct compression or hemostatic bandage.
Multiple bleeding in different spots that don’t allow the optimal application of direct pressure.
Patients with severe external hemorrhages in extremities that require urgent ventilatory support or airway maintenance.
The best way to control bleeding depends on a series of factors such as the victim’s state, and the magnitude and severity of hemorrhage, the proximity to a health department with surgical solving capacity, the simultaneous number of those injured, accessibility of human resource and transportation means, as well as emergency shock unit health personnel training on damage control, since they are who provide the primary assistance in a hospital12.
Airway
The polytraumatized patient should always be considered as “difficult airway”. It is mandatory to administer supplemental oxygen in these patients to maintain oxygenation and prevent hypoxemia.
Airway obstruction is the main cause of avoidable mortality in polytrauma. It is produced in unconscious patients due to the tongue falling towards the pharynx and in conscious patients due to the obstruction of airway by blood, vomit, edema, foreign objects or food remains13.
The first phase of identification is characterized by three alerts:
Cervical alert
Is referred to the immediate cervical stabilization in which the assistant will keep the head-neck-trunk aligned and immobilized in a neutral position. The neck collar will be placed only if the patient’s present situation does not require intubation.
If necessary, the instrumental management of the airway will proceed with bimanual immobilization and once the airway is established the collar will be placed.
It is fundamental to remember that the selective restriction of spinal movements is what has proven to have better results in children (NICE 2016).
The collar should always be removed to evaluate the neck.
State of consciousness alert
Consists in determining the state of alert in a child, as a general norm every conscious patient that speaks or breaths has a permeable airway. If the patient were unconscious, with abnormal respiratory sounds, irregular breathing or retractions, the instrumental airway management is initiated immediately13.
Airway alert
If the airway is obstructed, we proceed to unblock through secretion aspiration or removal of foreign objects. To maintain a permeable airway, oropharyngeal cannulas are used. Keep in mind a semi-conscious or conscious patient may present with vomiting or laryngospasms with risk of bronco aspiration. If no improvement is observed, the orotracheal intubation is indicated, with which definite airway control is achieved. Remember it is indicated in different phases of our initial evaluation of the polytraumatized pediatric patient. Remember to apply a rapid sequence of intubation with premedication. The intubation should be performed by removing the collar, immobilizing the cervical column in a bimanual manner and always using a bougie type guide. Other advanced airway management options, in case of not achieving orotracheal intubation, include supraglottic devices, preferably those who posteriorly co-adjuvate the orotracheal intubation (SALT, LMA Fastrack devices, laryngeal tubes), as well as cricothyrotomy in extreme cases14,15.
R. Respiration
Secure the airway and proceed to immobilize the neck. Then evaluate the patient’s pulmonary function (oxygen and ventilation) and detect signs of severe respiratory insufficiency. Evaluate the organ position to detect the presence of cyanosis, neck congestion, thorax dilation, dyspnea and pulmonary air quality. If symptoms of persistent respiratory insufficiency are present, it is important to rule out the presence of tension pneumothorax before intubating16. In this stage, it is critical to detect fatal thoracic lesions such as tension pneumothorax, open pneumothorax, or massive pneumothorax. Due to the rapid progression, the diagnosis must be based on clinical evidence, without waiting for radiologic confirmation for treatment. The older the patient and the lower the complexity, the less resistant the pneumothorax is. The ventilator may convert a simple pneumothorax into a tension pneumothorax, and whenever there is a suspicion of tension pneumothorax during hospital treatment, drainage over the puncture should be prioritized (NICE 2016). If this can’t be obtained and/or if the condition is not permitted, an immediate thoracocentesis should be performed ono the second intercostal space, midclavicular line, with a 14 or 16 G catheter coupled to a water seal or Helmich valve that fulfills the same function. In case of open pneumothorax, it should be sealed to avoid tension pneumothorax and convert it to simple pneumothorax that is controlled as previously described. Massive hemothorax correspond to the presence of blood in the pleural cavity causing hemodynamic instability (> 20 cc / kg / hr or > 25% blood volume in pediatric patients). Treatment consists of placing a thoracic drainage tube in the fifth intercostal space along the midaxillary line and perform a potent volume replacement15.
C. Circulation. Hemodynamic management of damage control.
After securing that the airway is not obstructed and verifying oxygenation and ventilation, the patient’s circulatory system should be evaluated. First, confirm the location where the compression device was previously placed, since the hemostatic gauze prevents bleeding. If the bleeding continues, evaluate the placement of a second tourniquet. If the first is used or a fabric device for compression, the first tourniquet should be placed. If the patient is amputated, the tourniquet should be immediately applied16,17. Posteriorly, the patient should be clinically evaluated to detect signs of hypovolemic shock and classify their severity (compensated or uncompensated/ hypotensive), Analyze the following to determine severity:
Central and peripheral pulses
Capillary refill (<4 seconds)
Temperature
Heart rate
Arterial pressure
Currently, the standard vascular Access for patients with multiple critical lesions is the immediate placement of osteoclysis (intraosseous water). If time and patient conditions allow, two peripheral lines should be cannulized in the forearm and the use of short and great caliber jelcos are recommended. When the prior method fails, the third line is the percutaneous line in the femoral vein18 Once the venous line is canalized, whether intravenous or intraosseous, a blood sample should be collected for a complete blood count, cross tests for transfusion and glycemia, the latter using destroxtis to rule out hyperglycemia or hypoglycemia. The gold standard treatment for traumatic shock from hypovolemia caused by hemorrhage is the immediate administration of reconstituted blood (NICE 2016). The possibility of applying protocols for balanced massive transfusion should be evaluated using the ABC classification of massive transfusion. If signs of shock appear, administer liquids to improve the hemodynamics19. Restrictive fluid replacement should be managed, meaning if you do not count on blood use hypertonic saline solution 3% at a dose of 5-10 cc kg in 20 minutes as a second option to avoid the phenomenon of reperfusion and instability of the already formed clots (“popping the Clot” phenomenon), three doses, if you cannot apply this option then use saline solution 0,9% at a dose of 20 cc kg during 20 minutes20. If hemorrhage is not controlled begin management of permissive hypotension and delayed resuscitation with hypertonic saline solution 3% from 5 to 10 cc/ kg in 20 minutes with the purpose of avoiding complications such as consumption coagulopathy, reperfusion syndrome and internal compartment syndrome. Permissive hypotension method is contraindicated when the patient presents cranioencephalic traumatism and younger than 5 years of age17. In patients 5 to 17 years of age with a head lesion, hypotension permissive measures are prohibited17. When each solution bolus is finalized, evaluate the hemodynamic response of the patient exploring again the cardiovascular clinical data, as well as signs of third spacing (lung). If they don’t present signs of shock, liquids should be infused according to basal needs. Most probably the patient lost at least 20% of the circulating volume. If they don’t respond, a new bolus of corticoid and/or total blood transfusion should be assessed if they have it. Not yet controlled bleeding or occult bleeding should be searched for. In newborns and infants under 8 kg, intracranial bleeding alone may provoke severe hypovolemic shock as well as concomitant neurological involvement7,20.
H. Hypothermia
In children over 10 years of age, hypothermia implies a temperature under 35° and at younger ages hypothermia presents at higher temperatures. Neonates are considered hypothermic if they have a temperature under 37°. In polytraumatized patients, hypothermia has different etiologies, and hydric resuscitation can generate heat loss that is proportional to the mas of administered liquids and to the liquid temperature gradient in the patient. Hypothermia affects all body systems, adverse effects include arrhythmias, decrease in cardiac output and cardiac frequency, increase in vascular resistance, decrease in glomerular filtration rate and sodium absorption, central nervous system depression, etc. Nursing patients and newborns are transferred to a heat source as soon as possible to facilitate body temperature measurement21.
D. Neurological deficit (disability)/destroxtis (glycemia)/cranial lesion (head and eye injury) pain.
In this section we evaluate the four “D’s”:
Neurological deficit (Disability). Cranioencephalic traumatism causes primary and irreversible nervous damage as a direct result of impact. However, it is fundamental to avoid secondary lesion due to hypovolemia, hypotension, hypoxia and hypercapnia.
The standard evaluations are:
Pupil evaluation through the light pupil response (size, response capacity and symmetry), is an indicator of brainstem function.
The AVDI (alert, verbal, pain, unconsciousness) pediatric response scale21,22allows evaluation of the cerebral cortex function, and
the Glasgow scale (eye opening, motor and verbal responses) determines the level of consciousness and neurological state of the pediatric patient. If the patient has a score < 8 they should be intubated.
Intracranial hypertension signs should be sought:
Anisocoria
Bradycardia / tachycardia
Hypertension
Pupilar hyporeactivity
Decerebrate or decorticate posturing.
Rapid Glasgow decrease
If they exist, hypertension empiric treatment is begun with hypertonic saline solution at 3% (5 to 10 cc/kg).
Glycemia (Destroxtis): If the patient presents hypoglycemia, a bolus of glucose solution at 10% at 2 cc kg dose should be immediately administered.
Ocular deficit: Ocular lesion, if necessary, cover them with dressings and wait for eye wash during the second evaluation.
Pain: Pain management is very important since its damaging effects such as oxygen consumption, energy, glucose and increase in intracranial pressure. Therefore, it is necessary to manage pain as soon as possible.
E. Exposure
The final step in the primary evaluation is to prepare for the second evaluation: The patient must be exposed, their clothing should be removed entirely. Once undressed, a quick exploration will be performed to localize lesions that cannot wait to be diagnosed during a second exploration, such as amputations, deformities, exposed fractures or lesions in internal organs. The patient’s evaluation must be complete (anterior and posterior), the necessary safety measures must be taken during the patient’s mobilization in order to avoid lesions21.
F. FAST, Pharmaceuticals and Family
The name of the FAST ultrasound derives from the English acronym Focused Abdominal Sonography for Trauma. It is used in the United States since 1990 and its main objective is to detect free fluid in the abdominal cavity of patients with closed abdominal traumatisms. Six areas are assessed:
Hepatorenal recess or Morrison’s pouch
Splenorenal recess
Bilateral paracolic gutters
Pelvis
Pericardium
Some centers assess the thorax searching for pleural effusion or pneumothorax.
The indications for the FAST exam include: Abdominal, blunt or penetrating chest trauma, undifferentiated shock and/or hypotension (as part of the Rapid Ultrasound for Shock and Hypotension (RUSH) exam).
This study, if available, is performed in the first evaluation and in the shock trauma center. In this phase, the early administration of coadjuvant drugs is administered, such as tranexamic acid, analgesics, and, if necessary, antibiotics, blood components, etc. Pain and anxiety management in polytraumatized pediatric patients is very important in reducing morbimortality. We begin with ketorolac, fentanyl or buprenorphine depending on the type of lesion and the main hemodynamic and neurologic clinical condition. Only if necessary, should first line antibiotics be started since one of the causes of death in intensive therapy is sepsis. However, starting antibiotics is not indicated in traumatic lesions, such as burns, if there is no clinical or laboratory information that suggests the presence of an infectious process.
FAMILY
During this time, we should inform the child’s family about the patient’s condition avoiding minimizing or hiding their state. The informed consent has been framed mainly through the legal and moral philosophy languages. Therefore, the informed consent legally protects patients from aggressions and lesions in the form of unwanted medical interventions. The patient’s state of consciousness is important when receiving information about the illness and treatment they require. If there is a condition that prevents the acceptance or refusal for treatment, this information may be presented to a legal representative who will make the decision with respect to the medical steps to follow. However, the legal standards that apply to obtaining the informed consent vary from one jurisdiction to another and its interpretation continues evolving. Some jurisdictions use the reasonable person standard, while others use the oldest reasonable physical person standard, therefore, it is important that clinicians determine the precise standard used in their jurisdiction and adapt their practice in an orderly fashion. This way, according to the laws of the nation in which they reside, it is important to consider life and the wellbeing of the pediatric patients above any religious discipline against treatment refusal. Blood transfusions generally are performed in the child’s benefit. The information given to the patient is an important aspect, it should be of quality and understandable to the patient, family member or legal representative, avoiding complex terminology, with the purpose that the family member or legal representative, in the case of pediatric patients, make the best decision. Therefore, the informed consent is basically a communication process and has to focus on reassuring the patient, to benefit them and face their illness the best way possible18,19.
Secondary evaluation
The secondary evaluation only initiates once the primary evaluation has been completed and the life-threatening lesions have been treated. If, during an examination, any decline is detected, they need to go back to go over the primary evaluation. A detailed clinical history and physical exam, diagnostic imaging, and problem identification of the significant lesions must be performed. Throughout the evaluation, standard precautions for blood or fluid transmitted infections must be observed. The MEASIRT methodology may be performed to easily remember the steps to be followed18,19.
Monitoring
While the team leader performs the primary evaluation, the patient should be monitored since this gives a quick notion of the response to the treatment administered.
Cephalocaudal exploration
Head and face. Examination of the head allows to discover a hematoma in the scalp, a depression or laceration in the cranium. The scalp and osseous segment lacerations may only be identified through careful palpation, which is why palpation of the scalp is important, as well as assessing all facial expressions, including the orbit, superior and inferior mandible and the nose.
Neck. Should be carefully examined, palpated and immobilized. A lesion in the cervical column should be assumed until the contrary is proven, which will be studied through diagnostic imaging of X-rays or computerized tomography. Swelling and acute pain in the throat should be searched for.
Thorax. Thoracic lesions, in order of frequency in a pediatric patient, are pulmonary contusions, rib fractures, pneumothorax and hemothorax. They should be identified and treated as an emergency in the primary evaluation of massive hemothorax, tension pneumothorax and cardiac tamponade. Pleural effusion due to tension pneumothorax and cardiac paralysis should be detected and treated urgently during the initial evaluation. The entire thoracic wall should be palpated to detect crepitation (subcutaneous emphysema) and sensitivity. The area above the sternum and the clavicles requires spatial attention since the fractures that affect these bones may suggest a significant force and the need for evaluation searching for intrathoracic lesions. Evaluate the presence of respiratory distress, abnormal respiratory and cardiac sounds. Inspect if there is a hematoma related to the safety belt. An X-ray should be taken and in the event of pleural effusion or pneumothorax, the necessary drainage should be performed.
Abdomen. Subtle signs of closed abdominal trauma from hollow or solid organ should be searched for. These signs are most frequent in the unconscious patient, and we should consider that its absence does not rule out the possibility of a serious abdominal lesion.
Extremities. The extremities should be evaluated to assess contusions, bleeding, crepitations, deformities, wounds, etc. The integrity of the joints not lesioned by the active and passive movements.
Back. The patient should be mobilized in blocks to search for back and spine lesions. If neck lesions have not been ruled out, patient should be immobilized.
Complete neurological exploration. Neurological exploration must be evaluated in a complete manner reevaluation the initial exploration:
Consciousness level
Pupil
Glasgow scale
Cranial pairs
Mobility and muscular tone
Sensitivity
Osteotendinous reflexes
(Focused clinical history)/Care documentation
In the clinical history we should consider the probability of damage and the forever trauma mechanism and when they are known. The SAMPLE mnemonic application, (signs/symptoms, allergies, medication, prior clinical history, last time they ate or drank and events that led to the current illness), serves to identify antecedents and discomfort that the child presents. This information is useful in determining the decline in respiratory, neurological or cardiovascular function21,22.
Referral
Taking into account the findings in the first and second physical evaluation we should assess the referrals to diverse practitioners (pediatric surgeons, neurosurgeons, orthopedics, intensive therapy, plastic surgeons, etc.). Therefore, the decision to transfer a polytraumatized patient after stabilization depends on the availability of these resources21,22.
Periodic reevaluation/ X-rays/tomography
During the treatment and stabilization phase, it is necessary that the patient continue with monitoring indicated in the initial exploration. However, we should pay attention to a reiterated patient reevaluation. The polytraumatized pediatric patient may evolve in a rapid form which is why the periodic reassessment is important to promptly detect any complication that may arise(24). Once the patient is stabilized, specific diagnostic imaging tests may be performed, such as imaging, x-rays/ tomography (Tertiary evaluation).
Transfer
Once we’ve obtained the initial stabilization of a patient with multiple traumas, we should consider asking the trauma hospital to begin treatment of the lesion in primary phase (surgical). The adequate hospital should be assessed. Mainly in our means, it will be a tertiary hospital or a hospital center with experience in pediatric polytraumatized patient management. When the transfer is performed, it will be when the patient finds themselves the most stable possible and have been accepted by the receiving hospital center. A bidirectional communication between the sending hospital, the receiving party and the transport team is required.24,25).
CONCLUSIONS
Polytrauma is characterized by the presence of multiple lesions and/or a single lesion that is life-threatening, being the cause of death at the moment of the accident or hours later in 30% of patients due to the complications caused by hemorrhage, hypovolemia or hypoxia. The approach in these patients requires directing the attention to the early reestablishing of vital functions of the child performing procedures leading to avoid damage due to coagulopathies, acidosis, hypothermia, hypoglycemia and hypoxia, which is performed through the concept of immediate resuscitation or damage control resuscitation. To perform a general evaluation or clinical approach, we recommend the attention outline with a general evaluation that includes the Pediatric Evaluation Triangle for a diagnostic, rapid and brief evaluation, based on visual and auditive patient guidelines, the Primary Evaluation through the MARCHDF system, for the evaluation and treatment of hemorrhages, airway, breathing, circulation, hypothermia, neurological deficit, cranial lesion, glucometer, exposure and FAST ultrasound and administration of coadjuvant medications in the treatment (hemorrhage control, analgesia). Later a Secondary Evaluation is performed through the MESIRT system that allows a complete patient assessment and exploration from head to toe performing a cephalocaudal exploration and monitoring, for such a clinical history is directed through a pneumonic SAMPLE (signs/symptoms, allergies, prior Medication, previous pathology, food/liquids and last meal and event origin). Referrals are done for a multidisciplinary approach. A periodic re-assessment should be performed, with studies and conclude with the movement of the patient to an adequate trauma center to start damage control in phase 1 which corresponds to the center with greater experience in the management of the pediatric polytraumatized patient. The procedures since the prehospital management to the treatment in the last instance, requires an effective, fluid, bidirectional communication, and a multidisciplinary follow-up (Figure 4).
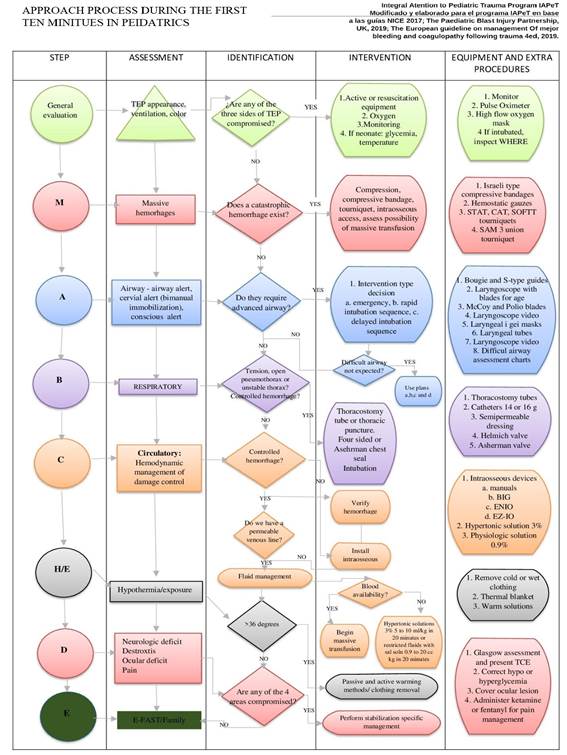
Figure 4: MARCH-D Protocol. Whenever a phase is observed, the clinical data assessed and its therapeutic approach in order of priority. This protocol is directed for damage control caused by the mortal triad of trauma before damage control surgery and in order for admission there to be the most stable possible.
REFERENCES
1. Spinella PC, Borgman MA, Azarow KS. Pediatric trauma in an austere combat environment. Crit Care Med. julio de 2008;36(7 Suppl):S293-296. doi: 10.1097/CCM.0b013e31817da99f. [ Links ]
2. Thompson T, Stanford K, Dick R, Graham J. Triage assessment in pediatric emergency departments: a national survey. Pediatr Emerg Care. agosto de 2010;26(8):544-8. doi: 10.1097/PEC.0b013e3181ea718e [ Links ]
3. Jayashree M, Singhi SC. Initial assessment and triage in ER. Indian J Pediatr. septiembre de 2011;78(9):1100-8. doi: 10.1007/s12098-011-0411-3. [ Links ]
4. Dieckmann RA, Brownstein D, Gausche-Hill M. The pediatric assessment triangle: a novel approach for the rapid evaluation of children. Pediatr Emerg Care. abril de 2010;26(4):312-5. doi: 10.1097/PEC.0b013e3181d6db37. [ Links ]
5. Corrales AY, Starr M. Assessment of the unwell child. Aust Fam Physician. mayo de 2010;39(5):270-5. Disponible en: https://pubmed.ncbi.nlm.nih.gov/20485711/ [ Links ]
6. Kleinman Monica E., Chameides Leon, Schexnayder Stephen M., Samson Ricardo A., Hazinski Mary Fran, Atkins Dianne L., et al. Part 14: Pediatric Advanced Life Support. Circulation. 2 de noviembre de 2010;122(18_suppl_3):S876-908. doi: https://doi.org/10.1161/CIRCULATIONAHA.110.971101 [ Links ]
7. Griffin E. Conducting triage research: lessons learned in a pediatric emergency department. J Emerg Nurs. Mayo de 2011;37(3):258-60. doi: 10.1016/j.jen.2011.02.015 [ Links ]
8. Berg Marc D., Schexnayder Stephen M., Chameides Leon, Terry Mark, Donoghue Aaron, Hickey Robert W., et al. Part 13: Pediatric Basic Life Support. Circulation. 2 de noviembre de 2010;122(18_suppl_3):S862-75. doi: https://doi.org/10.1161/CIRCULATIONAHA.110.971085 [ Links ]
9. Soyer T, Deniz T, Akman H, Hançerliogullari O, Türkmen F, Cesur O, et al. The impact of Pediatric Trauma Score on burden of trauma in emergency room care. Turk J Pediatr. agosto de 2009;51(4):367-70. Disponible en: https://pubmed.ncbi.nlm.nih.gov/19950845/ [ Links ]
10. Ortega García JP, Chávez Ramírez MA, Covarrubias Vela JA, Díaz Hernández AE, Guzmán Núques RE, Espino Núñez JS, et al. Propuesta de protocolo de hemorragia masiva. An Méd México DF. 2018;63(2):111-6. Disponible en: https://biblat.unam.mx/es/revista/anales-medicos-mexico-d-f/articulo/propuesta-de-protocolo-de-hemorragia-masiva [ Links ]
11. Nystrup KB, Stensballe J, Bøttger M, Johansson PI, Ostrowski SR. menatric trauma patients: a review of the literature. Scand J Trauma Resusc Emerg Med [Internet]. 15 de febrero de 2015 [citado 13 de mayo de 2021];23. Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4336766/ [ Links ]
12. Cunningham A, Auerbach M, Cicero M, Jafri M. Tourniquet usage in prehospital care and resuscitation of pediatric trauma patients-Pediatric Trauma Society position statement. J Trauma Acute Care Surg. octubre de 2018; 85(4):665-7. doi: 10.1097/TA.0000000000001839. [ Links ]
13. Gehri M, Flubacher P, Chablaix C, Curchod P. [Pediatrics. The PAT: a simple and rapid tool for the assessment of the severely ill or injured child]. Rev Med Suisse. 12 de enero de 2011;7(277):64-6. Disponible en: https://pubmed.ncbi.nlm.nih.gov/21309178/ [ Links ]
14. Dieckmann RA. Pediatric education for prehospital professionals. Jones & Bartlett Learning; 2006.15. Santillanes G, Gausche-Hill M. Pediatric airway management. Emerg Med Clin North Am. noviembre de 2008; 26(4):961-75, ix. doi: 10.1016/j.emc.2008.08.004. [ Links ]
15. Santillanes G, Gausche-Hill M. Pediatric airway management. Emerg Med Clin North Am. noviembre de2008;26(4):961-75, ix. doi: 10.1016/j.emc.2008.08.004. [ Links ]
16. Strehlow MC. Early identification of shock in critically ill patients. Emerg Med Clin North Am. febrero de 2010; 28(1):57-66, vii. doi: 10.1016/j.emc.2009.09.006. [ Links ]
17. 17. Cuenca CM, Borgman MA, April MD, Fisher AD, Schauer SG. Validation of the age-adjusted shock index for pediatric casualties in Iraq and Afghanistan. Mil Med Res [Internet]. 2 de julio de 2020 [citado 14 de mayo de 2021];7. Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7331217/ [ Links ]
18. Gale HL, Borgman MA, April MD, Schauer SG. Pediatric Trauma Patient Intensive Care Resource Utilization in U.S. Military Operations in Iraq and Afghanistan. Crit Care Explor. diciembre de 2019;1(12):e0062. doi: 10.1097/CCE.0000000000000062. [ Links ]
19. Hargrave JM, Pearce P, Mayhew ER, Bull A, Taylor S. Blast injuries in children: a mixed-methods narrative review.BMJ Paediatr Open. 1 de septiembre de 2019;3(1):e000452. doi: http://dx.doi.org/10.1136/bmjpo-2019-000452 [ Links ]
20. Naylor JF, April MD, Roper JL, Hill GJ, Clark P, Schauer SG. Emergency department imaging of pediatric trauma patients during combat operations in Iraq and Afghanistan. Pediatr Radiol. mayo de 2018;48(5):620-5. doi: 10.1007/s00247-017-4065-9 [ Links ]
21. Pannell D, Poynter J, Wales P, Tien H, Nathens A, Shellington D. Factors affecting mortality of pediatric trauma patients encountered in Kandahar, Afghanistan. Can J Surg. 1 de junio de 2015;58(3):S141-5. doi: 10.1503/cjs.017414 [ Links ]
22. Milwood Hargrave J, Pearce P, Mayhew ER, Bull A, Taylor S. (2019 Sep ). Blast injuries in children: a mixed-methods narrative review.. BMJ Paediatr Open, 3;3(1), 6-11. doi: 10.1136/bmjpo-2019-000452 [ Links ]
23. Naylor JF, April MD, Roper JL, Hill GJ, Clark P, Schauer SG. (2018 May). Emergency department imaging of pediatric trauma patients during combat operations in Iraq and Afghanistan.. Pediatr Radiol, 48(5):, 620-625. Doi: 10.1007/s00247-017-4065-9 [ Links ]
24. Wegner Araya A. Reanimación con control de daños en el trauma grave pediátrico. Rev Chil Pediatr.2018;89(1):118-27. Doi: 10.4067/S0370-41062018000100118 [ Links ]
Received: May 02, 2021; Accepted: June 14, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
