










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.3 Lima jul./set. 2021
http://dx.doi.org/10.25176/rfmh.v21i3.3921
Clinical case
Bilateral breast carcinoma in visceral crisis
1Instituto de Investigación de Ciencias Biomédicas, Facultad de Medicina Humana, Universidad Ricardo Palma, Lima- Perú.
2. Unidad de investigación Oncológica Hospital María Auxiliadora
3. Dirección de control y prevención de Cáncer - MINSA, Lima - Perú
4. Institución Liga Contra el Cáncer Lima-Perú.
Bilateral breast carcinoma is rare and infrequent, it is good to define if it occurs synchronously or metachronously, to define if the lesion in the second breast is metastasis or a primary tumor using pathological criteria, the state and clinical condition. For the prognosis and specialized treatment to follow. We present the case of a patient with ECIV breast cancer due to contralateral breast metastasis in a state of visceral crisis at debut, with pathological anatomy of grade 2 infiltrating ductal carcinoma of the breast, absent in situ component in both breast, RE (70%) , RP (80%), Cerb2 negative, Ki67 30% in the right breast and RE (100%) RP (80%) Cerb2-Ki67 20% left breast. A chest-abdomen-pelvis tomography was performed, showing pleural effusion. bilateral and large volume ascites. It was decided to start treatment with systemic chemotherapy, reaching a complete radiological and clinical response. After achieving good control of the disease, the first hormonal line will be sought.
Keywords: Infiltrating ductal breast carcinoma; contralateral metastasis; visceral crisis. (fuente: MeSH NLM).
INTRODUCCION
Breast cancer is the most common neoplasm in women and the 5th leading cause of death around the world1 Bilateral breast cancer (BCC) has an incidence of approximately 0.7 to 1.8% 2,3 and even in other literature it is mentioned that there is a risk of presenting BCC of approximately 0.5% to 0.75%. 4.5. It is good to define if it occurs synchronously <1 year according to Heron, or metachronously> 1 year, to define if the lesion in the 2nd breast is a metastasis or another primary cancer using the Chaudary pathological criteria6,7. We know that having a BCC have worse prognosis than unilateral breast cancer8,9. All this is important both in the prognosis and specialized treatment9,10
CASE REPORT
We present the case of a 48-year-old patient with no significant family oncological history, no relevant pathological history, with a 2-year illness time characterized by asthenia and abdominal pain, who was admitted by emergency due to exacerbated dyspnea, marked abdominal distention, whose preferential physical examination revealed tumors in both breasts, both on the right side of approximately 5 x 5 cm with an axillary ganglion more or less 2x2 cm with little hard motility, and a tumor in the left breast measuring 5 x 5 cm without palpable ganglion. On examination of the chest and lung: decreased vesicular murmur at the base with increased vocal vibrations, at the abdominal level a wave sign +, displaceable dullness, in lower limbs edemas marked with fovea ++ / +++ was evidenced. A biopsy of both breast lesions was performed, the result being in the right breast was infiltrating ductal carcinoma of the breast, grade 2, component in situ absent with immunohistochemistry in which the estrogen receptor (ER) + 70%, progesterone receptor (PR) + 80%, Cerb2 negative, Ki67 30%; and in the left breast, infiltrating ductal carcinoma of the breast, grade 2, absent in situ component with immunohistochemistry RE (100%) RP (80%) Cerb2-Ki67: 20% (Figure 2y 3). The emergency analysis showed hypoxemia due to AGA: pO2 55 mmHg, gauze ascites fluid study (blood albumin / ascites gradient (GASA)) <1.1, negative ascites fluid PAP, leukocyte hemogram 5300 / mm3 (neutrophils 43.2%) with rest of the hemogram, coagulation profile and biochemistry in normal values, for this reason it was decided to perform a chest-abdomen-pelvis tomography, showing large volume ascites and bilateral pleural effusion. (Figura 1) Considering that the patient was found in visceral crisis at that time: respiratory failure, ascites and massive pleural effusion and considering it a case of clinical stage IV infiltrating lobular breast cancer due to contralateral breast metastasis according to the criteria of Chaudary et al., In crisis state visceral, for which it is decided to start systemic chemotherapy of the 1st line Adriamycin - Cyclophosphamide (Cyclophosphamide 600 mg / m2 and doxorubicin 60 mg / m2) 4 courses + 12 courses Paclitaxel (80mg / m2) weekly with contrast tomographic control chest, abdomen and pelvis (09-01-18): showing complete remission of ascites, pleural effusion. (Figure 4). Bone scan (GGO) 10/17/18: no evidence of metastatic disease. Clinically, there is a reduction in tumor size in both breasts, remission of respiratory failure, and ascites. Being a luminal B patient: she began treatment with tamoxifen on a palliative basis with stable disease at the time.
DISCUSSION
48-year-old female patient, native and from Lima, with an illness time of approximately 2 years characterized by asthenia and abdominal pain. Whoever is admitted as an emergency due to exacerbated dyspnea, marked abdominal distention. On examination of the chest and lung: decreased vesicular murmur at the base with increased vocal vibrations compatible with pleural effusion clinically, at the abdominal level a wave + sign was evidenced, displaceable dullness compatible with ascites clinically, in the emergency laboratory tests hypoxemia due to AGA and related to the respiratory condition already described. Ascites fluid study (GASA) <1.1, negative ascitic fluid PAP, with this it should be remembered that the serum albumin gradient - ascites: GASA, allows us to identify if the ascites is due to portal hypertension or other causes. It is obtained by subtracting the value of serum albumin minus the albumin of the ascites fluid from samples obtained on the same day. If it is higher than 1.1g / dl it may be due to cirrhosis, cardiac ascites, Budd-Chiari syndrome or liver metastasis; if it is <1.1 g / dl, it may be due to peritoneal carcinomatosis, peritoneal tuberculosis, nephrotic syndrome or pancreatic ascites. For all these reasons, it was decided to perform a chest, abdomen and pelvic tomography with contrast, showing bilateral pleural effusion and marked ascites compatible with the aforementioned symptoms. (Figure 1). Preferential physical examination revealed tumors in both breasts both on the right side with axillary ganglion present with little hard motility, and a tumor in the left breast without palpable ganglion, which suggests that the suggestive symptoms could be due to a neoplastic process. Therefore, it was decided to perform core biopsy in both breasts with the following histology: infiltrating carcinoma, intermediate histological grade, infiltrating lobular carcinoma, ER +. RP +, Cerb b2 -, Ki 67 left breast: 20%, Ki 67 right breast: 30% both absence of in situ component, and negative cadherin, for which we are facing a case of: clinical stage infiltrating lobular breast cancer stage IV due to metastases of the contralateral breast. We consider CS IV based on the pathological criteria of Chaudary et al. In bilateral breast cancer there is an incidence of approximately 0.7 to 1.8% 2,4,5. It is good to define if it occurs synchronously <1 year according to Herón, or metachronously> 1 year, to define if the lesion in the 2nd breast is a metastasis or 2nd primary cancer using the Chaudary pathological criteria6,7. We know that having a BCC is a worse prognosis than unilateral breast cancer8,9. All of this is important both in the prognosis and specialized treatment9,10. We define whether it is really a metastasis or a second primary tumor using the Chaudary criteria7, which are summarized in 4 items:
Which describes whether the lesion in the 2nd breast has an in-situ component, makes us suspect a second primary cancer
If we have a higher degree of differentiation, it is suggestive of a second primary cancer.
If we have a different histology, let's think about a second primary cancer
Last but not least: if we have similar histologies in both breasts and with the absence of locoregional or distant metastasis, it could indicate a second primary cancer
Let's report what we have in our patient:
In both breasts component in situ absent,
Similar degree of differentiation in both tumors according to pathology
Histology in both breasts as evidenced by a negative single row and cadherin pattern indicating invasive lobular carcinoma
Faced with the fourth criterion, our patient presented a hard, non-mobile axillary adenopathy that inferred a probability of locoregional metastasis without even taking into account ascites and pleural effusion, which could be considered as distant metastasis
For all the above, we classify it as a clinical stage IV breast cancer due to the contralateral breast We show marked intensity estrogen receptors as evidenced in right breast (RB), left breast (LB), as well as similar progesterone + receptors in both breasts, negative cerb-b2 in RB and LB, ki67 30% in RB and 20% LB : cataloging Luminal B breast cancer Our patient is in visceral crisis state because she presents an organ dysfunction characterized by signs, symptoms and laboratory tests (dyspnea, ascites, surge sign +, respiratory failure and hypoxemia demonstrated by AGA) that show marked clinical deterioration plus a visceral commitment, which forces us to act quickly and effectively11. Treatment depends on the clinical stage at the time of diagnosis. Considering a metastatic CS IV , it should be mentioned that in patients with hormone receptor (HR) positive metastatic breast cancer, starting chemotherapy before hormone therapy has not been shown to increase survival as evidenced in the Cochrane meta-analysis with studies by Dixon, Tashiro and Taylor in their respective investigations12,13. We have to take in consideration that currently in RH positive metastatic breast cancer the standard first-line treatment is hormone therapy + cyclin CDK 4-6 inhibitors, which has been shown to significantly prolong progression-free survival in this scenario. With great examples such as the clinical benefit of palbociclib as initial therapy for postmenopausal women with estrogen receptor positive, epidermal growth factor 2 negative (ER +, HER2-) metastatic breast cancer, the phase 3 PALOMA-2 study demonstrated that the combination of palbociclib + letrozole vs letrozole improved disease-free survival of 24.8 months vs 14.5 months, showing a net benefit of 10 months HR 0.58 CI (0.46-0.72), it should also be noted that the combination of palbociclib and letrozole exceeded two years of PFS (progression-free survival), making it the best first line in this population of women. Benefit was also mentioned in the MONALEESA-7 study with hormone therapy + ribociclib with 23.8% vs 13.0% PFS HR 0.55 (0.44-0.69).14,15 However, there is a scenario in which the probability of starting chemotherapy is indicated: only in the visceral crisis state according to the NCCN 2020 guidelines12 In our patient we started with 4 AC cycles and 12 weekly Paclitaxel cycles, showing disappearance of ascites and pleural effusion Figure 4 GGO, no metastasis was evident In September 2018 we started with tamoxifen until now with good disease control There is little evidence and reported cases of contralateral metastatic breast cancer at the time of diagnosis as debut, using the criteria of Chaudary et al., and that they have responded to chemotherapy as first line in a state of visceral crisis, prolonging their disease-free survival, which our work contributes to the scientific and academic literature.
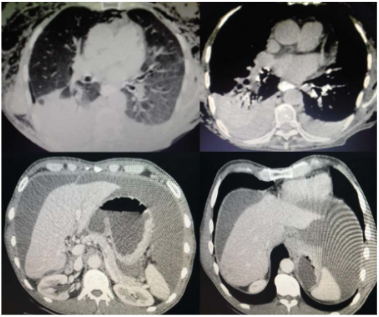
Figure 1 Contrast chest, abdomen and pelvis tomographic study 07-11-17 showing bilateral pleural effusion, no pulmonary nodular lesions, free fluid in extensive degree in the intraperitoneal cavity, liver without solid or cystic focal nodular lesions, retroperitoneum does not show adenopathy no lumps.
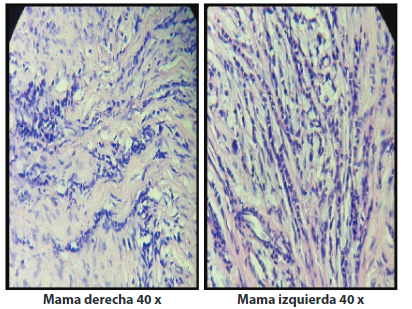
Figure 2A Cellular microscopy of the breast tissue is observed: cell populations in a single-row pattern in both right and left breast corresponding to invasive lobular carcinoma (H-E staining, 40 X).
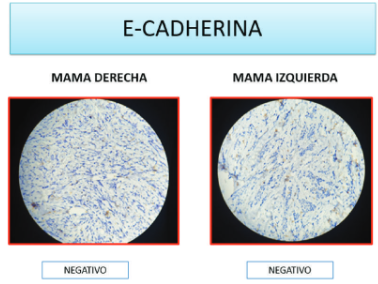
Figure 2B Negative E-cadherin is observed in both breasts, a calcium-mediated glycoprotein related to epithelial cell adhesion, the absence of which is compatible with lobular carcinoma.
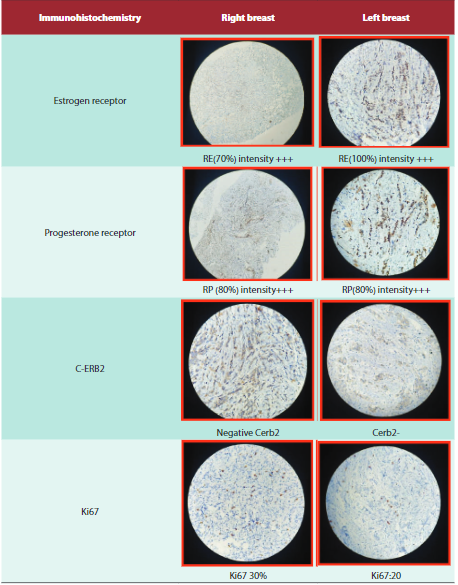
Figure 3 Immunohistochemical test for breast cancer, divided into the following categories: estrogen receptor (ER) / progesterone receptor (PR) positive as luminal A, ER / RP / Her-2 positive as luminal B, Her-2 positive (Her-2 array) and triple negative (basal-like). It is also considered that those tumors that only express hormone receptors, but the expression of the cell proliferation marker or Ki-67 is greater than 14%, are classified as luminal B. All this is important for both the prognosis and the respective treatment.
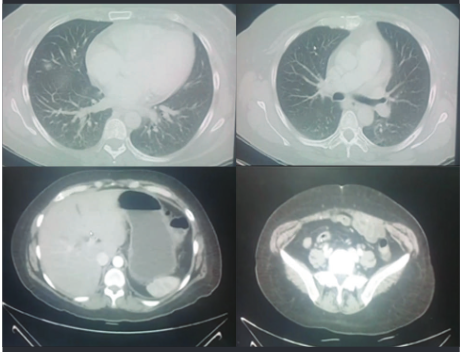
Figure 4 Tomographic study of the thorax, abdomen and pelvis, 01-09-18, where pulmonary fields with density and preserved configuration are evidenced, not showing interstitial thickening, consolidation process, or pulmonary nodules and without evidence of pleural effusion, no fluid is observed in the peritoneal cavity, remnants of organs and pelvis within normal limits.
CONCLUSIONS
It is important to differentiate between a second primary vs metastatic breast cancer due to the respective prognostic and therapeutic implications.
In patients with metastatic RH + breast cancer, the standard treatment is hormone therapy + CDK 4/6 inhibitors according to the bibliography and guidelines.
Patients with visceral crisis are candidates for first-line treatment with CT.
There are few reported cases, it is necessary to deepen in more studies in breast cancer with contralateral metastases.
REFERENCES
1. International Agency of Research on Cancer . GLOBOCAN 2018:Estimated Cancer Incidence , Mortality and Prevelance worldwide in 2018 .Disponible en: http://www.who.int/features/factfiles/cancer/en/ [ Links ]
2. Begg CB, Ostrovnaya I, Geyer FC, Papanastasiou AD, Ng CKY, Sakr RA, et al. Contralateral breast cancers: Independent cancers or metastases? International Journal of Cancer. 2018;142(2):347-56.. doi:10.1002/ijc.31051 [ Links ]
3. Alkner, S., Tang, M.E., Brueffer, C. et al. Contralateral breast cancer can represent a metastatic spread of the first primary tumor: determination of clonal relationship between contralateral breast cancers using next-generation whole genome sequencing. Breast Cancer Res 17, 102 (2015). Doi: https://doi.org/10.1186/s13058-015-0608-x [ Links ]
4. Takahashi H, Watanabe K, Takahashi M, Taguchi K, Sasaki F, Todo S. The impact of bilateral breast cancer on the prognosis of breast cancer: a comparative study with unilateral breast cancer. Breast Cancer 2005;12:196-202. DOI:10.2325/jbcs.12.196 [ Links ]
5. Kurian AW, McClure LA, John EM, Horn-Ross PL, Ford JM, Clarke CA. Second primary breast cancer occurrence according to hormone receptor status. J Natl Cancer Inst. 2009 Aug 5;101(15):1058-65. doi: 10.1093/jnci/djp181. PMID: 19590058; PMCID: PMC2720990. [ Links ]
6. Liu Y, Dong C, Chen L. The clinicopathological features of second primary cancer in patients with prior breast cancer: Medicine. abril de 2017;96(16):e6675. doi:10.1097/MD.0000000000006675 [ Links ]
7. Chaudary MA, Millis RR, Hoskins EOL, Halder M, Bulbrook RD. Bilateral breast cancer: A prospective study of disease incidence. Br J Surg 1984;71:711-4 [ Links ]
8. Carmichael AR, Bendall S, Lockerbie L, Prescott R, Bates T. The long-term outcome of synchronous bilateral breast cancer is worse than metachronous or unilateral tumours. Eur J Surg Oncol 2002;28:388-91. doi:10.1053/ejso.2002.1266 [ Links ]
9. Chuba PJ, Hamre MR, Yap J, Severson RK, Lucas D, Shamsa F, et al. Bilateral risk for subsequent breast cancer after lobular carcinoma in-situ: analysis of surveillance, epidemiology, and end results data. J Clin Oncol 2005;23:5534 -41 DOI: 10.1200/JCO.2005.04.038 [ Links ]
10. Heron DE, Komarnicky LT, Hyslop T, Shwartz GF, Mansfield CM. Bilateral breast carcinoma: risk factor and outcomes for patients with synchronous and metachronous disease. Cancer 2000 Jun; 88(12): 2739-50 [ Links ]
11. Sbitti Y, Slimani K, Debbagh A, Mokhlis A, Kadiri H, Laraqui A, Errihani H, Ichou M. Visceral Crisis Means Short Survival Among Patients With Luminal A Metastatic Breast Cancer: A Retrospective Cohort Study. World J Oncol. 2017 Aug;8(4):105-109. doi: 10.14740/wjon1043w.. PMID: 29147444; PMCID: PMC5650006. [ Links ]
12. National Comprehensive Cancer Network, NCCN Practice Guidelines in Oncology-v.3.2020. Disponible en: http://www.nccn.org/professionals/physician_gls/PDF/breast.pdf (9 May 2020, date last accessed) [ Links ]
13. Systemic treatment of metastatic breast cancer in women: Chemotherapy - UpToDate [Internet]. [citado 10 de mayo de 2020]. Disponible en: https://www.uptodate.com/contents/systemic-treatment-of-metastatic-breast-cancer-in-women-chemotherapy [ Links ]
14. Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365:1687. doi: 10.1016/S0140-6736(05)66544-0. [ Links ]
15. Finn RS, Martin M, Rugo HS, Jones S, Im S-A, Gelmon K, et al. Palbociclib and Letrozole in Advanced Breast Cancer. N Engl J Med. 17 de noviembre de 2016;375(20):1925-36. DOI: 10.1056/NEJMoa1607303 [ Links ]
Received: January 10, 2021; Accepted: May 19, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
