










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.4 Lima out./dez. 2021
http://dx.doi.org/10.25176/rfmh.v21i4.3609
Original article
Clinical epidemiological characteristics of patients diagnosed with SARS-CoV-2. Hospital I Florencia De Mora Essalud - La Libertad, 2020
1Universidad Cesar Vallejo, Perú.
Introduction:
the SARS-CoV-2 pandemic affected a large part of the population of La Libertad, among them, the population of Florencia de Mora whose hospital played an important role in the care of patients diagnosed with COVID-19.
Objective:
to determine the epidemiological clinical characteristics of patients diagnosed with SARS-CoV-2 treated at the care center.
Methods:
Retrospective observational descriptive study, with a population of 2622 patients treated in the COVID-19 triage, taking into account the molecular test and the rapid serology test for the detection of SARS-CoV-2.
Results:
SARS-CoV-2 was detected in 74.90% (1155) of patients. The months with the highest number of cases were June and July with 29.4% (340) and 37.4% (432), respectively. The predominant age group was 27- 59 years with 77.9% (900) and males with 57.5% (664). Regarding the clinical profile, the most frequent comorbidity was hypertension with 6.9% (80), obesity and overweight with 3.7% (43) and the most frequent symptoms were cough 62.9% (726) and odynophagia 55.7% (643).
Conclusions:
75 out of 100 screened patients had SARS-CoV-2, predominantly males, the age group of 27-59 years, hypertension, obesity and overweight as comorbidity, cough and odynophagia as the most frequent symptoms.
Keywords: Epidemiology; clinical picture; prevalence; SARS-CoV-2. (Source: MeSH NLM).
INTRODUCTION
SARS-CoV was responsible of the first pandemic in the XXI century which extended to 29 countries, reaching a mortality of 9.6%. The second pandemic was caused by MERS-CoV in 2021 in the Middle East, reaching a mortality of 34.4%1. In January 2020, the World Health Organization (WHO) declared a Health Emergency1,2and two months later it was considered a global pandemic due to COVID 193.
The human coronavirus strains are transmitted during winter and are responsible for the common cold1,4,5, otitis media in children, and pneumonia4,5, others are highly pathogenic, responsible for severe acute respiratory syndrome and Middle East Respiratory syndrome, respectively5,6.
SARS-CoV-2 is a beta-coronavirus that is transmitted by airway1,4, through fomites4, fecal oral7,8, and maternal-fetal9. The airway route is the main mode of transmission through flügge droplets that are spread up to two meters when speaking, sneezing, or coughing, and remain in the air for over 17 minutes1,4,10. The fomite mode of transmission is due to the virus remaining on smooth surfaces, from 4 hours1to 5 days depending on the type of material4,11; likewise, the oral fecal route is justified by the presence of viral RNA in feces even with a negative nasopharyngeal smear9and the result of infectious aerosols in the toilet, leading to a fomite transmission. Regarding maternal-fecal material, although it has not been proven yet, it still cannot be ruled out9.
The SARS-CoV-2 virus enters our organism through the nose, mouth or eyes, and enters the cell through the angiotensin-converting enzyme receptor (ACE2) 1,10-12; which is found in the pulmonary cytoplasmic membranes AT2, as well as ileum and colon cells, where they replicate11. The incubation period is 3 to 9 days, with the maximum viral load 2.5 days before symptoms appear10.
The most frequent symptomatology is fever, cough, myalgia or fatigue, dyspnea,1,8,10,11,13 sore throat, diarrhea, nausea and vomiting1,8,10,11, abdominal pain8,10,13, anorexia, dizziness, headache, altered sense of taste and smell9,11, arthralgias12, impaired consciousness, and urticarial or vesicular eruptions and purpura11. These are resolved after 10 to 15 days, but the viral shedding continues1.
Hospital I Florencia de Mora EsSalud was not included as a reference center for SARS-CoV-2 in Trujillo, however, due to the spread this virus has and the saturation of reference hospitals, it played an important role in offering health services for care of patients with COVID-19. Based on this, the objective of this study is to determine the clinical and epidemiological characteristics of patients diagnosed with SARS-CoV2.
METHODS
Design and area of study
A retrospective, observational, descriptive study, from the review of the archive management system of EsSalud, of patients treated in COVID triage in Hospital I Florencia de Mora (HIFM).
Population and sample
The population included 2622 patients defined as suspicious treated in COVID-19 triage of HIFM- EsSalud, La Libertad, during March to August 2020. We included patients diagnosed with COVID-19 confirmed with serologic or molecular testing, and patients who were not found during the control and follow-up calls were excluded, as well as those who requested voluntary withdrawal.
Variables and instruments
To assess the clinical epidemiological characteristics. confirmed cases were determined by positive serological and molecular tests, according to the definition in the official epidemiological alert. Regarding epidemiological characteristics, we considered age, origin and sex, while in clinical characteristics, symptoms and comorbidity were included.
Procedures
After obtaining permission from the institution, we proceeded to review the epidemiological sheets downloaded from NotiWeb, entering each sheet into a database for the epidemiological surveillance of each patient.
RESULTS
Out of a total of 2622 treated in COVID-19 triage of HIFM - EsSalud, only 58.85% (1543) underwent screening with the serological test method 94.5 % (1458), while molecular tests were 5.5% (85). Among the participants, 74.9% (1155) were diagnosed with SARS-CoV-2. It is important to mention that 5.54% (64) were hospitalized and 1.99% (23) died
Table 1. Distribution of patients screened for SARS-CoV- 2, according to test type, from the Hospital I Florencia de Mora - EsSalud - La Libertad, 2020.
| TYPE OF TEST | SEROLOGICAL | RT-PCR | TOTAL | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| REACTIVE | 65 | 4,2 | 1155 | 74.9 | |||
| IGM | 138 | 8,9 | |||||
| IGM/IGG | 719 | 46,6 | |||||
| IGG | 233 | 15,1 | |||||
| 1090 | 70,6 | ||||||
| NOT REACTIVE | 368 | 23,9 | 20 | 1,3 | 388 | 25,1 | |
| TOTAL | 1458 | 94,5 | 85 | 5,5 | 1543 | 100 | |
Source: Epidemiological area of HIFM
In Graph 1, we observe the COVID 19 cases according to month of screening, finding that the months with most cases were June and July, with 29.4% (340) and 37.4% (432), respectively.
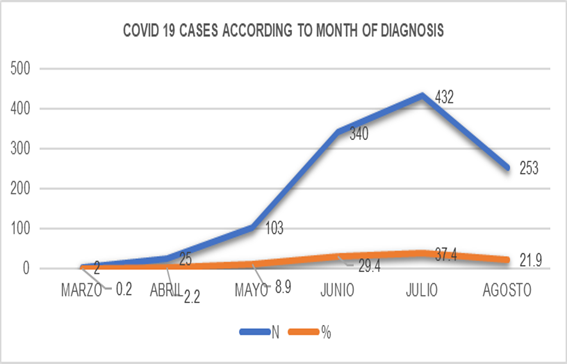
Graph 1: COVID-19 cases according to month of diagnosis in Hospital I Florencia de Mora, La Libertad, 2020
InTable 2, the variables age and sex pertaining to the epidemiological characteristics are found, with the most frequent age group 27-59 years, with 77.9% (900), and a mean age of 43.5 years ± 14.8. The most frequent sex was masculine, with 57.5% (664).
Table 2. Patients with SARS-CoV-2 diagnosis, according to age group and sex, of Hospital I Florencia de Mora - EsSalud, La Libertad, 2020.
| age group | Femenine | Masculine | Total | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| 1-4 | 1 | 0,1 | 1 | 0,1 | 2 | 0,2 |
| 5-11 | 4 | 0,3 | 5 | 0,4 | 9 | 0,8 |
| 12-17 | 7 | 0,6 | 9 | 0,8 | 16 | 1,4 |
| 18-26 | 37 | 3,2 | 41 | 3,5 | 78 | 6,8 |
| 27-59 | 371 | 32,1 | 529 | 45,8 | 900 | 77,9 |
| >60 | 71 | 6,1 | 79 | 6,8 | 150 | 13,0 |
| Total | 491 | 42,5 | 664 | 57,5 | 1155 | 100,0 |
Source: Epidemiological area of Hospital I Florencia de Mora.
26.1% of patients with SARS-CoV-2 presented some type of morbidity, with hypertension as the most frequent6.9% (80), obesity and overweight was found in second place, with 3.7% (43). 73.9 % (853) of patients did not present comorbidities.
Table 3. Distribution of 1155 patients with SARS-CoV-2 diagnosis, according to comorbidity, from Hospital I Florencia de Mora - EsSalud, La Libertad, 2020.
| COMORBIDITY | N | % |
|---|---|---|
| Hypertension | 80 | 6,9 |
| Obesity and overweight | 43 | 3,7 |
| Diabetes mellitus | 35 | 3,0 |
| Asthma | 32 | 2,8 |
| Hypertension and Diabetes Mellitus | 26 | 2,3 |
| Digestive System Disease | 14 | 1,2 |
| Interstitial lung and chronic obstructive disease | 12 | 1,0 |
| Cancer | 10 | 0,9 |
| Two or more diseases | 10 | 0,9 |
| Hypothyroidism | 9 | 0,8 |
| Neurologic Disease | 8 | 0,7 |
| Others | 8 | 0,7 |
| Osteomuscular Disease | 6 | 0,5 |
| Other respiratory diseases | 5 | 0,4 |
| Chronic renal disease | 4 | 0,3 |
| Without comorbidity | 853 | 73,9 |
| Total | 1155 | 100,0 |
Source: Epidemiological area of Hospital I Florencia de Mora
85% (982) of patients with SARS-CoV-2 presented symptoms. Symptoms according to age group are shown in table 4, the most frequent was cough with 62.9% (726) and odynophagia with 55.7% (643). In the age group of 6-11 years, the most frequent symptom was nasal congestion with 0.4% (5), in the 18-26 years group was odynophagia 4.1% (47), while in the 12-17 years age group, 27- 59 years, and over 60 years was cough with 0.9% (10), 47.6% (550) and 10.4% (120), respectively.
Table 4. Distribution of 1155 patients with SARS-CoV-2 diagnosis, according to symptoms and age group, of Hospital I Florencia de Mora EsSalud, La Libertad, 2020.
| Symptoms | 1-5 years | 6-11 years | 12-17 years | 18-26 years | 27-59 years | >60 years | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| Cough | 1 | 0,1 | 4 | 0,3 | 10 | 0,9 | 41 | 3,5 | 550 | 47,6 | 120 | 10,4 | 726 | 62,9 |
| Odynophagia | 1 | 0,1 | 4 | 0,3 | 5 | 0,4 | 47 | 4,1 | 496 | 42,9 | 90 | 7,8 | 643 | 55,7 |
| General malaise | 1 | 0,1 | 3 | 0,3 | 7 | 0,6 | 33 | 2,9 | 427 | 37,0 | 88 | 7,6 | 559 | 48,4 |
| Headache | 0 | 0,0 | 2 | 0,2 | 6 | 0,5 | 41 | 3,5 | 415 | 35,9 | 60 | 5,2 | 524 | 45,4 |
| Fever | 1 | 0,1 | 3 | 0,3 | 5 | 0,4 | 29 | 2,5 | 385 | 33,3 | 71 | 6,1 | 494 | 42,8 |
| Myalgia | 0 | 0,0 | 3 | 0,3 | 5 | 0,4 | 24 | 2,1 | 370 | 32,0 | 67 | 5,8 | 469 | 40,6 |
| Chest pain | 1 | 0,1 | 1 | 0,1 | 4 | 0,3 | 18 | 1,6 | 266 | 23,0 | 44 | 3,8 | 334 | 28,9 |
| Nasal congestion | 1 | 0,1 | 5 | 0,4 | 7 | 0,6 | 30 | 2,6 | 254 | 22,0 | 37 | 3,2 | 334 | 28,9 |
| Difficulty breathing | 0 | 0,0 | 0 | 0,0 | 1 | 0,1 | 5 | 0,4 | 211 | 18,3 | 72 | 6,2 | 289 | 25,0 |
| Diarrhea | 1 | 0,1 | 2 | 0,2 | 2 | 0,2 | 8 | 0,7 | 182 | 15,8 | 26 | 2,3 | 221 | 19,1 |
| Anosmia | 0 | 0,0 | 0 | 0,0 | 5 | 0,4 | 13 | 1,1 | 177 | 15,3 | 18 | 1,6 | 213 | 18,4 |
| Ageusia | 0 | 0,0 | 0 | 0,0 | 5 | 0,4 | 13 | 1,1 | 177 | 15,3 | 18 | 1,6 | 213 | 18,4 |
| Nauseas | 0 | 0,0 | 0 | 0,0 | 0 | 0,0 | 5 | 0,4 | 79 | 6,8 | 12 | 1,0 | 96 | 8,3 |
| Joint pain | 0 | 0,0 | 0 | 0,0 | 1 | 0,1 | 0 | 0,0 | 50 | 4,3 | 11 | 1,0 | 62 | 5,4 |
| Abdominal pain | 0 | 0,0 | 1 | 0,1 | 2 | 0,2 | 4 | 0,3 | 22 | 1,9 | 3 | 0,3 | 32 | 2,8 |
| other | 0 | 0,0 | 1 | 0,1 | 4 | 0,3 | 0 | 0,0 | 17 | 1,5 | 7 | 0,6 | 29 | 2,5 |
Source: Epidemiology area of Hospital I Florencia de Mora.
DISCUSSION
In this study we performed a screening of 1543 (58.9%) people who visited the differentiated triage for COVID-19, in Hospital I Florencia de Mora. We found that 75 out of 100 patients screened had COVID-19, a result similar to 70.07% (192) reported in the study by Villagrán-Olivas K (Mexico)14, and greater than 22.66% (349) by Vila-Córcoles A. (Spain)15. Both studies opted for the molecular test for the screening since they were sensitive and specific, as well as because they had no cross reactivity with respiratory viruses16. However, Villagrán-Olivas K14used a population of 242 suspected cases, while Vila-Córcoles A15, despite included a population of 79 071 patients, only screened 2% (1547).
However, our country opted to diagnose with rapid serologic tests that are economical, easy and simple to use16, these detect IgM and IgG antibodies, present in up to 40% in the first week from the start of symptoms and reach up to 100% by day 1517. Despite that Sánchez C (Lima-Perú)18used the same diagnostic test, he included health personnel in his study population, and reported 25.6% (1112). This difference may occur since the population studied was more exposed, unlike our study, in which we opted to wait for isolation time for screening, which would allow for more confirmed cases to be presented.
With regard to months with greater reported cases, these were June and July with 29.4% (340) and 37.2% (432). These results coincide with the months of greater positivity in the department of La Libertad19.
Among the epidemiological characteristics, the most frequent sex was masculine with 57.5% (664). This result is consistent with the reports by Villagrán-Olivas K (Mexico)14 with 59.38% (114), Ferrer J. (Cuba) with 52.7(71)20in hospitalized patients, and Llaro-Sánchez M(Lima-Perú) con 69.57 %16,21in deceased patients. However, they differ with what was found by Vila-Córcoles A. (Spain)15, Sánchez C. (Lima-Peru)18and Guzmán-Del Giudice O. (Lima-Peru)22, who found that the feminine sex was the most frequent with 59% (206) ,71.7% (797), and 52%13, respectively. This is because men are more predisposed to contracting COVID-19 due to their greatest habit to tobacco, concomitant diseases23,24, and exposure to risk determinants, however, these results are not conclusive23.
The most frequent age group were adults, with 77.9% (900). These findings coincide with Villagrán-Olivas K (Mexico)14, Sánchez C (Lima-Peru)18and Guzmán-Del Giudice O(Lima-Peru)22, while studies with deceased patients such as Llaro-Sánchez M(Lima-Peru)21and Escobar G(Lima-Peru)25the frequent age group were older adults. This difference is due because older adults have a high fatality rate due to their immune system deficit, associated to concomitant diseases, which would justify the frequency of studies with deceased patients26, while in young adults are more immersed in the labor and social sector, which justifies their frequency in our study.14
Within the clinical profile, the most frequent comorbidity was hypertension with 6.9% (80). This coincides with Vila-Córcoles A. (Spain)15and Escobar G. (Lima-Peru)25; while it differs from that reported by Villagrán-Olivas K (Mexico)14and Sánchez C (Lima-Peru)18, where the most frequent comorbidity was obesity. This is because hypertensive patients consume medications such as ACE inhibitors and ARA which increase the levels of ACE2, receptors also found in the heart and blood vessels, which would facilitate the entry of virus into cells12.
In our study, obesity was the second most frequent comorbidity with 3.7% (43), unlike 33.3% (64) referred in the work by Villagrán-Olivas K., who carried out the study in Mexico, a co9untry where obesity is found among the first places in the world14, while Sánchez C. carried out their study with health personnel, who due to their routine they had no healthy habits, which is why obesity is present among them.
Among the symptoms, the most frequent were cough with 62.9% (726), odynophagia 55.7% (643), and general malaise 48.4% (559). This result differed from Villagrán-Olivas K. (Mexico)14and Guzmán-Del Giudice O. (Lima-Peru)23, who reported fever and cough as the most frequent symptoms. This is because they included hospitalized patients in their sample. Likewise, it partially coincides with the review by Ferrer J. (Cuba)20, whose study reported cough and fever in patients of all ages, as in this research.
We must mention the insufficient supply of molecular tests as a study limitation, which could have conditioned a sub registry of positive cases of COVID-19 in the 2622 patients who were screened in the differentiated triage. Likewise, the follow-up of some patients was difficult because they did not answer the telephone or because they were hospitalized.
REFERENCES
1. Ruiz A, Jiménez M. SARS-CoV-2 y pandemia del síndrome respiratorio agudo (COVID-19). Ars Pharm [internet].2020 [Acceso 21 de agosto 2020]; 61(2):63-79. DOI:10.30827/ars.v61i2.15177 [ Links ]
2. Wanden C, Sanz J. La Hospitalización a Domicilio en la enfermedad del COVID-19. Hosp Domic [internet]. 2020[Acceso 02 de septiembre 2020];4(2): 55-57.DOI: 10.22585/hospdomic. v4i2.105 [ Links ]
3. Castro R. Coronavirus, una historia en desarrollo. Rev Med Chile [internet].2020[Acceso 29 de agosto 2020]; 148: 143-144. DOI:10.4067/s0034-98872020000200143 [ Links ]
4. Carot F. Complicaciones neurológicas por coronavirus y Covid 19. Rev Neurol [internet]. 2020[Acceso 23 de agosto 2020]; 70:311-322. DOI: 10.33588/rn.7009.2020179 [ Links ]
5. Bonilla K, Villamil W, Rabaan A, Rodríguez A. Una nueva zoonosis viral de preocupación global: COVID-19, enfermedad por coronavirus 2019. IATREIA [internet]. 2020[Acceso 25 de agosto 2020]; 33(2). Disponible en: http://www.redalyc.org/articulo.oa?id=180563251001 [ Links ]
6. Aragón R, Vargas I, Miranda M. COVID-19 por SARS-CoV-2: La nueva emergencia de salud. Rev. Mex Pediatr [internet] 2019[Acceso 27 de agosto 2020]; 86(6): 213-218.DOI: 10.35366/91871 [ Links ]
7. Ding S,Liang J . Is SARS-CoV-2 also an enteric pathogen with potential fecal-oral transmission? a COVID-19 Virological and Clinical Review. Gastroenterology[internet] .2020[Acceso 5 de septiembre 2020];159:53-61. DOI:10.1053/j.gastro.2020.04.052 [ Links ]
8. Parra V, Flórez C, García F, Romero C. Síntomas gastrointestinales en la enfermedad por COVID-19 y sus implicaciones en la Enfermedad Inflamatoria Intestinal. Rev Colomb Gastroenterol [internet]. 2020[Acceso 7 de septiembre 2020];35(1). DOI: 10.22516/25007440.532 [ Links ]
9. Hijona J, Carballo A. Fernández A, Bermúdez M, Expósito J. ¿Existe transmisión materno-fetal del SARS-CoV-2 durante la gestación? Rev Clin Esp. [internet] 2020[Acceso 10 de septiembre 2020]. DOI:10.1016/j.rce.2020.06.001 [ Links ]
10. Sepúlveda V,Waissbluth S,González C.Anosmia y enfermedad por Coronavirus 2019 (COVID-19): ¿Qué debemos saber?Rev Otorrinolaringol Cir Cabeza Cuello [Internet]. 2020; [citado 20 septiembre 2020 ]80: 247-258. DOI: 10.4067/S0718-48162020000200247 [ Links ]
11. Marcial J. El SARS-CoV-2 y otros virus emergentes y su relación con la inocuidad en la cadena alimentaria. Scientia Agropecuaria [internet].2020[Acceso 15 de Septiembre 2020] 11(2): 267 - 277 Disponible en:https://revistas.unitru.edu.pe/index.php/scientiaagrop/article/view/2929/3095 [ Links ]
12. Salazar M,Barochiner J,Espeache W,Ennis I.COVID-19, hipertensión y enfermedad cardiovascular.Hipertens riesgo Vas [Internet].2020[citado 12 de noviembre 2020]; 37(4):176-180. DOI:10.1016/j.hipert.2020.06.003 [ Links ]
13. Cobas-Planchez L, Mezquia-de-Pedro N, Armenteros-Terán SS. Características clínicas de pacientes con sospecha de COVID-19 ingresados en el hospital "Frank País García", La Habana. Rev electron Zoilo [Internet]. 2020 [citado 17 septiembre 2020];45(4). Disponible en: http://revzoilomarinello.sld.cu/index.php/zmv/article/view/2339 [ Links ]
14. Villagrán-Olivas K, Torrontegui-Zazueta L,Entzana-Galindo A. Características clínico-epidemiológicas de pacientes de COVID-19 en un Hospital de Sinaloa, México. Rev Med UAS [Internet].2020[citado 15 octubre 2020].10(2). DOI:10.28960/revmeduas.2007-8013.v10. n2.003 [ Links ]
15. Vila-Córcoles A, Ochoa-gondar O,Torrente-Fraga C,Vila-Rovira A,Satué-Gracia E, Hospital-Guardiola I, el al.Evaluación de la incidencia y perfil de riesgo de covid-19 según comorbilidad previa en adultos =50 años del área de tarragona. Rev Esp Salud Pública [Internet]. 2020[citado 19 Octubre 2020];94:1-15.Disponible en : https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/resp/revista_cdrom/VOL94/ORIGINALES/RS94C_202006065.pdf [ Links ]
16. Gestión de las intervenciones individuales y colectivas para la promoción de la salud y prevención de la enfermedad. Lineamientos para el uso de pruebas moleculares RT-PCR, pruebas de antígeno y pruebas serológicas para SARS-CoV-2 (COVID-19) en Colombia.Bogota[Internet] -2020[citado 24 Octubre 2020].Disponible en: https://www.minsalud.gov.co/Ministerio/Institucional/Procesos%20y%20procedimientos/GIPS21.pdf [ Links ]
17. Aguilar P, Enríquez Y, Quiroz Valencia E, León Pareja A. Pruebas diagnósticas para la COVID-19: la importancia del antes y el después. Horiz Med [Internet] .2020[citado 26 Octubre 2020];20 (2).Disponible en: http://www.scielo.org.pe/scielo.php?pid=S1727-558X2020000200014&script=sci_arttext [ Links ]
18. Sánchez C. "Características clínicas y epidemiológicas de personal sanitario con covid-19 del primer nivel de atención de Lima norte, Abril - Junio, 2020". Tesis para optar en grado de bachiler.Trujillo[Internet] -2020[citado 22 Octubre 2020].Disponible en: http://repositorio.upao.edu.pe/bitstream/upaorep/6620/1/RE_MEHU_JOANNA.VILLARREAL_RELACI%c3%93N.ENTRE.%c3%8dNDICE.ALB%c3%9aMINA.CREATININA.PROTEINURIA.24HORAS .DIABETES.MELLITUS.TIPO2.pdf [ Links ]
19. Gerencia regional la Libertad. Sala situacional COVID-19:26-03-2021/La Libertad. Disponible en: https://www.facebook.com/GeresaLaLibertad/photos/pcb.3902444056461042/3902444009794380 [ Links ]
20. Ferrer J, Sánchez E, Mendoza A, Del Río G, Figueredo D. Caracterización clínica y epidemiológica de pacientes confirmados con la COVID-19 en la provincia de Santiago de Cuba. MEDISAN [Internet] 2020[citado 29 octubre 2020]; 24(3):474. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192020000300473 [ Links ]
21. Llaro-Sánchez M, Gamarra-Villegas B, Campos-Correa K. Características clínico-epidemiológicas y análisis de sobrevida en fallecidos por COVID-19 atendidos en establecimientos de la Red Sabogal-Callao 2020. Horiz Med [Internet] .2020[citado 31 de octubre 2020]; 20(2): e1229. DOI :10.24265/horizmed.2020.v20n2.03 [ Links ]
22. Guzmán-Del Giudice O, Lucchesi-Vásquez E,Trelles-De Belaúnde M,Pinedo-Gonzales R, Camere-Torrealva M, Daly A, et al. Características clínicas y epidemiológicas de 25 casos de COVID-19 atendidos en la Clínica Delgado de Lima. Rev Soc Perú Med Interna [Internet]. 2020[citado 02 de noviembre 2020];33(1). DOI:10.36393/spmi. v33i1.506 [ Links ]
23. Castellanos-Torres E, Tomás J, Chilet-Rosell E. COVID-19 en clave de género COVID-19 en clave de género.Gac Sanit [Internet]. 2020. [citado 04 de noviembre 2020];34(5):419-421.Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7190475/ [ Links ]
24. Ruiz M. Las estadísticas sanitarias y la invisibilidad por sexo y de género durante la epidemia de COVID-19. Gac Sanit [Internet]. 2020. [citado 06 de noviembre 2020]. DOI:10.1016/j.gaceta.2020.04.008 [ Links ]
25. Escobar G, Matta J, Ayala R, Amado J. Características clínico epidemiológicas de pacientes fallecidos por covid-19 en un hospital nacional de Lima, Perú Rev Fac Med Hum [Internet].2020. [citado 08 de noviembre 2020] 20(2).Disponible en : http://www.scielo.org.pe/scielo.php?pid=S2308-05312020000200180&script=sci_arttext [ Links ]
26. Blanco-Tarrioa E, Blanco Sánchez G. Atención primaria y residencias de ancianos: a propósito de la COVID-19. SEMERGEN. [Internet] 2020[citado 10 de noviembre 2020];46 (S1): 33- 41.DOI: 10.1016/j.semerg.2020.06.003 [ Links ]
Received: January 20, 2021; Accepted: September 05, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
