










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.4 Lima out./dez. 2021
http://dx.doi.org/10.25176/rfmh.v21i4.3936
Original article
Socioeconomic characteristics and costs of rare and orphan diseases in Peru, 2019
1Facultad de Medicina Humana, Universidad Ricardo Palma. Lima, Perú.
2Universidad Continental. Lima, Perú.
Introduction:
The rare and orphan diseases (ROD) constitute a current challenge due to the lack of investigation.
Objective:
Describe the socioeconomic characteristics of rare and orphan diseases (ROD) in Peru, 2019.
Methods:
Descriptive observational design. The information was obtained from FISSAL administrative records, and an intentional sample of 20 patients was taken to carry out the questionnaire on ROD. For the economic records, a review of the public budget of the MEF was made. The data analysis was descriptive and inferential.
Results:
There were 454 patients with a total of 49 ROD; of these, the most representative age groups were schoolchildren and young adults (18% each), and the most frequent diagnosis was Tetralogy of Fallot (22%). The questionnaire on ROD reports a median of 7 months in the delay of diagnosis and between 3 and 5 doctors were visited. Likewise, 30% considered that it generated a high to very high expense. It was calculated that the ROD budget constitutes 2.25% of the total budget for high-cost diseases. Likewise, the ROD budget was different between 2014 and 2019.
Conclusions:
The population with ROD in Peru is not large; however, it requires greater attention to access to health services and a greater budget allocation.
Keywords: Rare diseases; cost of illness; economics; health economics; Peru (Source: MeSH NLM).
INTRODUCTION
Rare and orphan diseases (ROD) represent a challenge today, as they only have 40 years of research1. Their denomination of "rare" assumes that they constitute as low frequency diseases, an idea that changes when evaluating them all together, since an approximate of 7000 ROD is calculated for which the World Health Organization (WHO) affirms that they affect around the 7% of the world population under the definition of a prevalence of less than 0.65% or 1%.1-5The latest analysis, based on epidemiological data from Orphanet, showed that the prevalence of ROD is 3.5% -5.9% of the world population, which is equivalent to 300 million affected people6.
In Peru, in 2011, Law No. 29698 was approved, declaring the treatment of people suffering from ROD of national interest and preferential care. They were grouped into categories: very high priority, high priority, low priority, and very low priority. In total, 399 diseases were identified. It should be noted that there is currently a new standard approved in 2019 by the Ministry of Health of Peru (MINSA) with RM No. 1075-2019 / MINSA, for the List of Rare or Orphan Diseases7.
It is important to highlight the medical journey traveled by patients with a rare disease (and their families) that, as Black et al. in his research, it is an odyssey8. The patient goes to a health center with the first symptoms, but the doctor does not suspect that it is a ROD, and thus, the patients will be referred to many specialists without obtaining answers and worsening their prognosis. For this reason, from the first level of care, improvements such as empathy, skills, and competencies for early diagnosis, good management and follow-up of the patient, and communication and research on the pathology, must be emphasized. There are few specific treatments for these pathologies. Still, specialized rehabilitation in ROD is essential since these patients have a lower quality of life than the general population, and some will present significant disabilities. Therefore, a rehabilitator who proposes personalized improvement techniques is essential.
The big problem is that there are no reliable epidemiological data on the prevalence and incidence in national and global populations to support public health interventions9. This study aims to determine the socio-economic characteristics of ROD in Peru and demographic factors, estimate the allocation of resources, and its economic impact in the country.
METHODS
Design and study area
An observational and descriptive design study was carried out, using data from Peru between the years 2014 and 2019.
Population and sample
The population corresponds to people affected by rare and orphan diseases in Peru, obtained from a database of administrative records of the health sector, the Intangible Solidarity Health Fund (FISSAL). In addition, a survey validated by Orphanet was carried out on an intentional sample of 20 people or relatives of people affected by rare and orphan diseases. For the economic part, the Ministry of Economy and Finance was consulted. People affected by diseases that do not appear in the list of 399 rare diseases identified in the country or that do not coincide with the respective ICD-10 were excluded.
Variable and instruments
The variables proposed were the sociodemographic characteristics of the patients (age, gender, origin, and comprehensive health insurance regime). As well as the time elapsed between the first symptom and the moment of diagnosis, how many doctors did they consult between the first manifestation of the disease and the diagnosis, if they gave you wrong diagnoses before the final diagnosis, if looking for the diagnosis required personal expense, if they received complete information on their illness, and if the patient or family received psychological support and if their origin was from the city of Lima or another (classified as "province"). Those inherent to the economic aspect of these diseases were total budget, budget execution, and unit cost.
The information was obtained from the database of administrative records of the health sector, FISSAL; A questionnaire validated by Orphanet was also taken into account. For the economic data, a review was made of the public budget of the Ministry of Economy and Finance, the Integrated Financial Administration System - Budget Monitoring (SIAF), available at: https://apps5.mineco.gob.pe/transparencia/Navegador/ default.aspx.
Procedures
The information on the economic aspect was obtained through the Modified Institutional Budget of the FISSAL-MINSA per year between 2014 and 2019. The figures shown in this budget are used to cover high-cost diseases such as Chronic Kidney Failure on dialysis, cancers, and rare and orphan diseases. For the first, approximately 60% is allocated, approximately 40% to the problem of cancer and only 2.25% to ROD (this is calculated with the data that for the year 2017 the allocation of resources for ROD was 5.8 million soles, that is, 2.25% of the total). Therefore, the ROD budget for each year was considered as 2.25% of the total budget for the same year.
On the other hand, the data collection of the Orphanet questionnaire was carried out through contact with the ESPERANTRA organization, which facilitated the meeting with patients to conduct interviews with them or their relatives in different hospital centers in Lima with different pathologies anonymously.
Statistical analysis
A descriptive analysis of the variables studied was carried out, using central tendency and dispersion measures for the quantitative variables and frequencies and percentages for the qualitative ones. Inferential analysis was carried out to compare the budget for ROD in 2015 against that of 2019; for this, the non-parametric Mann Whitney U test was used. SPSS version 25 and Microsoft Excel were used to process the database.
RESULTS
454 patients were registered with a total of 49 ROD according to the database in Peru. Regarding age, they were grouped: Newborns were 29 patients (6%), younger and older infants, 86 (10% and 9% respectively), preschoolers, 78 (17%), schoolchildren, 81 (18%), adolescents , 39 (8%), young adults, 80 (18%), mature adults, 36 (8%), older adults, 3 (1%) and no age, 22 (5%). Most were male (243, 54%). The origin of the majority was from the department of Lima (266, 59%), the one that follows in frequency is Junín with 20 patients (4%), 6% does not register origin, and the rest is distributed among the other Peruvian departments and the Callao province. The regimen by which patients are cared for the most part is subsidized (442.97%), SIS NRUS (6.1%), semi-contributory (3.1%), independent SIS, and independent insurance with 2 and 1 patients, respectively. Among the most diagnosed diseases are: Tetralogy of Fallot (102 patients, 22%), Systemic lupus erythematosus (87, 19%), gastroschisis (39, 9%), hemophilia A (34, 7%), osteogenesis imperfecta (30, 7%), the rest is divided among the other 44 listed diseases (Figure 1).
These diseases can be divided by their cause (if they are genetic or not); thus, 67% (33 diseases) are, but they only constitute 39% of all patients (177).
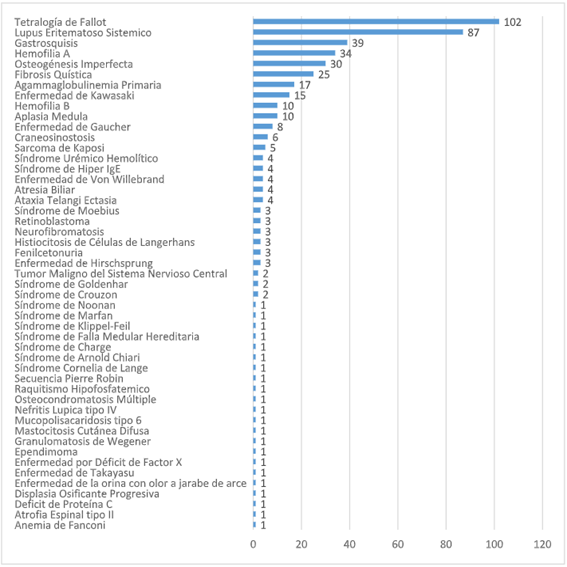
Figure 1: Diagnoses of people affected with rare and orphan diseases in Peru, 2017-2019 Source: FISSAL, own elaboration
On the other hand, the sociodemographic data obtained from the surveys carried out on an intentional sample of 20 people can be seen inTable 1.
Table 1. On the other hand, the sociodemographic data obtained from the surveys carried out on an intentional sample of 20 people can be seen in
| Time | Doctors consulted | diagnoses | Expenditure | Information | Psychological support | Origin |
|---|---|---|---|---|---|---|
| 6 MONTHS | 3 to 5 | Yes | Very High | Yes | No | Province |
| AT BIRTH | 1 | No | Little | No | Yes | Lima |
| AT BIRTH | 1 | No | Little | Yes | Yes | Province |
| 2 YEARS | 3 to 5 | No | Little | Yes | Yes | Province |
| 2.5 YEARS | 3 to 5 | Yes | Moderate | Yes | Yes | Province |
| 3 YEARS | 3 to 5 | Yes | High | Yes | No | Lima |
| 9 MONTHS | 3 to 5 | No | Moderate | Yes | No | Province |
| 3 YEARS | 3 to 5 | No | No | Yes | No | Province |
| 1 YEAR | 1 to 2 | No | Little | Yes | No | Lima |
| 1.5 YEARS | 1 to 2 | Yes | Very High | Yes | No | Province |
| 5 MONTHS | 3 to 5 | Yes | Moderate | Yes | No | Lima |
| 1 MONTH | 3 to 5 | No | High | Yes | No | Province |
| 6 MONTHS | 3 to 5 | No | Very High | Yes | Yes | Province |
| 2.5 YEARS | 3 to 5 | No | High | Yes | Yes | Province |
| 6 MONTHS | 1 to 2 | No | Moderate | Yes | Yes | Province |
| 6 MONTHS | 3 to 5 | No | Moderate | Yes | Yes | Province |
| 6.5 YEARS | 1 to 2 | Yes | Little | Yes | No | Province |
| 1 MONTH | 3 to 5 | No | Little | Yes | Yes | Lima |
| 1 YEAR | 3 to 5 | No | No | No | No | Province |
| 3 MONTHS | 1 to 2 | No | Moderate | No | Yes | Lima |
Time: elapsed between the first symptom and the moment of diagnosis. Doctors consulted: between the first manifestation of the disease and the diagnosis. Misdiagnoses - If you received misdiagnoses before the final diagnosis. Expense: level of expense caused by seeking the diagnosis. Information: if you received complete information about your illness. Psychological support: if the patient or family received psychological support. Province: City outside the department of Lima. Source: ORPHANET survey, own elaboration
As can be seen in the first column of this table, the longest time elapsed between the appearance of the first symptom and the moment of diagnosis was 6.5 years, followed by 3 years and in 2 cases was diagnosed at birth. The mean of these results is 1.33, which would mean that on average, the diagnosis would take 1 year and 3 months, but the standard deviation is 1.57, which warns of outliers that make the average unreliable. For this reason, the median is used, which was 0.6, which indicates that half of the patients after 7 months of the first symptom already had their diagnosis. 65% went between 3 to 5 doctors until they reached the definitive diagnosis and 35% from 1 to 2. Of the 20 patients surveyed, 6 of them (30%) gave a wrong diagnosis before reaching the final diagnosis. Regarding the disbursement made by each relative with a patient with the rare and orphan disease to reach the diagnosis only, it was: 10% did not generate expenses. 30% little, 30% moderate, and 30% high to very high. 85% of those surveyed received complete information about their illness or their family member at the time of diagnosis. Unlike the information about the disease, psychological support was given to only half of the patients and/or relatives. Most of the people interviewed came from the provinces of Peru (70%) and 30% from Lima.
InTable 2, you can see the total budget (Total FISSAL Budget) aimed at treating high-cost diseases and ROD, the executed budget, and the estimated budget allocated to ROD for each year, estimated from 2.25% of the total budget for that year.
Table 2. Total budget in soles of FISSAL compared to the budget directed to rare and orphan diseases, Peru 2014-2019
| Year | Total FISSAL Budget | Budget execution | Estimate (2.25% of the total budget) of the budget allocated to ROD |
|---|---|---|---|
| 2019 | 348 122 954 | 346,3 million | 7,8 million |
| 2018 | 418 523 371 | 398,2 million | 9,4 million |
| 2017 | 257 726 602 | 257,4 million | 5,8 million |
| 2016 | 192 943 209 | 192,8 million | 4,3 million |
| 2015 | 190 196 344 | 189,5 million | 4,2 million |
| 2014 | 152 196 791 | 151,7 million | 3,4 million |
ROD: Rare and orphan diseases. FISSAL: Intangible Solidarity Health Fund SOURCE: FISSAL, own elaboration
The budgetary data of FISSAL attributed to ROD (2.25% of the total) by departments in Peru for the years 2015 and 2019 were taken to analyze them comparatively. In the first instance, with the Kolmogórov-Smirnov test, it was possible to determine that the data do not have a normal distribution. For this reason, the nonparametric Mann-Whitney U test was used to face the budgets for ROD for 2015 compared to 2019, resulting in a p-value of 0.003; Therefore, the null hypothesis is rejected, that is, the median budget directed to ROD in the different provinces of Peru, is different between the years 2015 and 2019.
DISCUSSION
Sociodemographic data
The findings obtained show that 49 ROD of the 399 listed. In contrast to these figures, in the United States, they estimate that between 25 and 30 million patients have a ROD. In the European Union, it reaches approximately 27 to 36 million.9Few of the Latin American countries report accurate data, one of them is Colombia, which estimates in 2013 a total of 13,173 patients.10On the other hand, if we consider that 5 to 7% of the world's population suffers from some rare or orphan disease, when transferred to Peru, between 1.5 to 2 million would be affected11hypothetically, so the road is still long to have an accurate figure in the country.
Schoolchildren and young adults are the majority of patients, with 18% each. Still, if evaluated together, between newborns and all children, they add up to 60%, so these are diseases that occur more frequently in pediatric age. This agrees in part with the authors Carbajal and Navarrete,4who affirm that approximately 50% appears in pediatric age. Still, the highest prevalence is seen in adults due to excessive infant mortality due to these diseases.
54% were male. Similar to Colombia in a study on mortality due to ROD, it was found that 51.4% were men of all ages,12although with this it cannot be affirmed that the frequency of appearance is higher in them, since another study also in Colombia,10found that 53.96% of patients with ROD were women.
The origin of more than half of the patients is from the capital, Lima. The other departments have a very low percentage, but this may be due to their under-registration because it is difficult to diagnose and identify them even more outside the capital.
71% of patients are cared for in health facilities with a subsidized regime, which is the mechanism by which the population without the ability to pay access health services; in other words, it is the most impoverished population in the country.
In the literature, it is found that 72% of ROD are genetic and 70% of them begin in childhood,6the finding of the present study is close to this figure since 67% or 33 diseases are genetic such as hemophilia A and osteogenesis imperfecta , but if the distribution among the patients is seen, they only constitute 39% (177 patients), the other 277 suffer from congenital, acquired, multifactorial diseases or still of unknown etiology.
A study in China13chooses to study 7 rare diseases of their country, of which only Gaucher disease matches our list. Carbajal and Navarrete4list "the rarest and most curious diseases in the world," and only one coincides (Moebius syndrome). In the study of mortality due to orphan diseases in Colombia12cited above, gastroschisis is the only one that matches our list. It was a frequent cause of death in men and women; in still lack this data in our country. Of the most frequent pathologies according to the research of María Pareja,10two coincide with the findings of this study: Hemophilia A and Von Willebrand's disease, which occupy the fourth and fourteenth place in our results. In addition, his research includes the percentage of people with ROD with disabilities, which was 10.74% of the total, data that is not required in Peru either.
Several RODs can be diagnosed prenatally, which is important because it facilitates delivery and newborn care, ensures their well-being as much as possible, and suggests a better future prognosis.14Based on what was found in this study, of the 49 diseases, 13 can be diagnosed or at least suspected in utero (tetralogy of Fallot, gastroschisis, among others), by means of routine prenatal ultrasounds that refer to more specific tests, another 12 can be diagnosed prenatally if family history is known (hemophilia, primary agammaglobulinemia, cystic fibrosis, phenylketonuria, for example).
Neonatal screening is another way to detect ROD, in 2012 the law established interest for the screening of 6 pathologies in Peru15, of which phenylketonuria and cystic fibrosis are ROD on the list. Just for comparison, the United States has 32 diseases for newborn screening,16including the 2 diseases mentioned.
Based on the questionnaire, data were obtained that may or may not reflect the reality of rare and orphan diseases in the country, but it gives us a general idea.
First, it is obtained that the delay in diagnosis was up to 7 months for half of the patients, a fact that does not agree with the information collected in the bibliography; for the other half, it took from 1 to 6.5 years for the final diagnosis. Regarding the number of doctors who were seen, a marked majority is seen in the range of 3 to 5, without obtaining results greater than this. Regarding the impoverishment of the families, 12 people affirmed that reaching the diagnosis represented a moderate, high and very high expense, while for the other 8 it was little or none. At this point, it should be taken into account that the question only refers to the direct expenditure of the families to reach the diagnosis, without considering other expenses such as follow-up of the pathology, the price of medicines in some cases for life, rehabilitation, other products health and necessary care in addition to the high level of dependency that most of these patients have. In addition, the health insurance scheme they have was not included.
It is very important to provide complete information to the patient and/or relatives about the disease so that they take care of themselves and know what to expect from the disease in terms of complications and prognosis to make the quality of life the best possible, in addition to identifying the nature of the pathology so that, if it is the case of having genetic inheritance, that data can be known within the family, 85% of the people surveyed did receive this information; it was different in the case of psychological support since only half received it. Psychological support for the patient and their families is important, as in other cases as well, due to the high emotional impact, doubts, and fears that these diagnoses carry.
70% of the people surveyed came from the province, and in their entirety, they agreed that their stay in Lima was for some reason related to their illness or that of their relative, such as diagnosis, treatment or better conditions in terms of follow-up of their illness.
Budget
Regarding the budget, there is mostly an increasing trend as the years go by, and the highest amount assigned to ROD was that of 2018 with 9.4 million if we compare this figure with the 53.4 million soles that are required to pay for at least the first 8 diseases on the list, reflecting that it only covers 17.6%. Therefore, the insufficient budget allocated to ROD is evident.
Cost
Similar cases that denote the high cost of ROD can be found in the literature, for example, in Germany, in a study it is calculated that the cost of Annual treatment per patient with ROD is between € 27,811 and € 1,647,627 (S/. 104,013 and S/. 6,162,124), they also analyze the impact on the annual budget of ROD and ultra-rare in Europe, which it was on average € 677,975,264 (S/. 2,535,627,487) but of this amount, pharmaceutical spending only constituted 2.7% (0.7-7.8)17. Another study carried out a literature review (mostly European) that facilitated the prices of medicines for ROD, from which they concluded that the annual cost ranged from € 1,474 to € 912,000 (S/. 1,772 to 3,410,880) per patient, that is, an average of € 96,518 (S/. 360,977).18
The study has certain limitations since, being based on secondary sources, there could be errors regarding the diagnoses or underreporting. The comparison with other countries is minimal since the prevalence of the diseases can vary in different populations, thus being rare in some and more frequent in others, and there are few data worldwide. Its most significant strength is that it gives a broader vision of the reality that was had in Peru regarding ROD, which is a great step for public health.
REFERENCES
1. González-Lamuño Leguina D, Cruz Villalba J. Las enfermedades raras desde la Atención Primaria. AEPap. Curso de Actualización Pediatría 2017 [Internet]. Madrid: Lúa Ediciones 3.0; 2017. p.133-42. Disponible en: https://www.aepap.org/sites/default/files/133-142_enfermedades_raras.pdf [ Links ]
2. Quirland Lazo C, Castañeda Cardona C, Chirveches Calvache MA, Aroca A, Otárola Esteban M, Rosselli D. Modelos de atención en salud en enfermedades raras: revisión sistemática de la literatura. Gerenc Políticas Salud [Internet]. 2018; 17(34). Disponible en: http://revistas.javeriana.edu.co/index.php/gerepolsal/article/view/23128 [ Links ]
3. Carbajal Rodríguez L. Enfermedades raras. Acta Pediátrica México [Internet]. 2015;82 (6):207-10. Disponible en: https://www.medigraphic.com/pdfs/pediat/sp-2015/sp156f.pdf [ Links ]
4. Carbajal Rodríguez L, Navarrete Martínez JI. Enfermedades raras. Acta Pediátrica México [Internet]. 2015;36(5):369. Disponible en: https://ojs.actapediatrica.org.mx/index.php/APM/article/view/1057 [ Links ]
5. Cortés F. Las Enfermedades Raras. Revista Médica Clínica Las Condes [Internet]. 2015; 26(4):425-31. Disponible en: https://www.elsevier.es/es-revista-revista-medica-clinica-las-condes-202-articulo-las-enfermedades-raras-S0716864015000905 [ Links ]
6. Nguengang Wakap S, Lambert DM, Olry A, Rodwell C, Gueydan C, Lanneau V, et al. Estimating cumulative point prevalence of rare diseases: analysis of the Orphanet database. European Journal of Human Genetics [Internet]. 2019. Disponible en: http://www.nature.com/articles/s41431-019-0508-0 [ Links ]
7. Resolución Ministerial 1075-2019/MINSA. Documento técnico: Listado de Enfermedades Raras o Huérfanas [Internet]. 2019. Disponible en: https://cdn.www.gob.pe/uploads/document/file/426220/resolucion-ministerial-n-1075-2019-minsa.PDF [ Links ]
8. Black N, Martineau F, Manacorda T. Diagnostic odyssey for rare diseases: exploration of potential indicators [Internet]. London: Policy Innovation Research Unit, LSHTM. 2015; Disponible en: http://piru.lshtm.ac.uk/assets/files/Rare%20diseases%20Final%20report.pdf [ Links ]
9. Posada de la Paz M, Taruscio D, Groft SC. Rare Diseases Epidemiology: Update and Overview [Internet]. Cham: Springer International Publishing (Advances in Experimental Medicine and Biology; vol. 1031); 2017. Disponible en: http://link.springer.com/10.1007/978-3-319-67144-4 [ Links ]
10. Pareja Arcila ML. Situación actual de las enfermedades huérfanas en Colombia 2017. CES Derecho [Internet]. 2017;8(2):231-41. Disponible en: https://revistas.ces.edu.co/index.php/derecho/article/view/4493/2840 [ Links ]
11. Lizaraso Caparó F, Fujita R. Enfermedades Raras o Huérfanas, en Perú más huérfanas que raras. Horiz Méd Lima [Internet]. 2018;18(2):4-5. Disponible en: http://www.scielo.org.pe/pdf/hm/v18n2/a01v18n2.pdf [ Links ]
12. Martinez JC, Misnaza SP. Mortalidad por enfermedades huérfanas en Colombia, 2008-2013. Biomédica [Internet]. 2018;38(2):198-208. Disponible en: https://revistabiomedica.org/index.php/biomedica/article/view/3876 [ Links ]
13. Xin X-X, Guan X-D, Shi L-W. Catastrophic expenditure and impoverishment of patients affected by 7 rare diseases in China. Orphanet J Rare Dis. Diciembre de 2016;11(1):74. Disponible en: https://ojrd.biomedcentral.com/articles/10.1186/s13023-016-0454-7 [ Links ]
14. Reconret G, Ortega X, Pinto M. Diagnóstico prenatal y manejo perinatal en enfermedades raras. Rev Médica Clínica Las Condes [Internet]. 2015;26(4):432-41. Disponible en: https://cyberleninka.org/article/n/558304/viewer [ Links ]
15. Guio H, Poterico JA, Levano KS, Cornejo-Olivas M, Mazzetti P, Manassero-Morales G, et al. Genetics and genomics in Peru: Clinical and research perspective. Mol Genet Genomic Med [Internet]. 2018;6(6):873-86. Disponible en: https://pubmed.ncbi.nlm.nih.gov/30584990/ [ Links ]
16. Aguirre-López M, Sánchez IP, Arias AA, Giraldo ML, Velásquez-Velásquez EM, Franco JL, et al. Tamización neonatal para linfopenias congénitas y otras enfermedades raras en el mundo. Rev Esp Pediatr [Internet]. 2017;73(2):61-74. Disponible en: http://www.seinap.es/wp-content/uploads/2015/05/REP-73-2.pdf [ Links ]
17. Schlander M, Dintsios C-M, Gandjour A. Budgetary Impact and Cost Drivers of Drugs for Rare and Ultrarare Diseases. Value Health [Internet]. 2018;21(5):525-31. Disponible en: https://pubmed.ncbi.nlm.nih.gov/29753348/ [ Links ]
18. Korchagina D, Millier A, Vataire A-L, Aballea S, Falissard B, Toumi M. Determinants of orphan drugs prices in France: a regression analysis. Orphanet J Rare Dis [Internet]. 2017;12(1):75. Disponible en: https://ojrd.biomedcentral.com/articles/10.1186/s13023-016-0561-5 [ Links ]
Received: May 29, 2021; Accepted: July 09, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
