










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.4 Lima Oct./Dec. 2021
http://dx.doi.org/10.25176/rfmh.v21i4.3985
Clinical case
Parapharyngeal schawannnoma
1Hospital Nacional Edgardo Rebagliati Martins - Essalud - Lima- Peru.
Parapharyngeal tumor lesions present a low incidence, representing between 0,5 and 0,8% of all head and neck tumors. Approximately 80% show benign behavior. The uniqueness of these lesions derives from their complex anatomical situation and the symptoms with which they usually appear, being in most cases nonspecific and almost always derived from the compressive effect produced by the lesion on the oropharynx and the oropharynx. Schwannomas of the parapharyngeal space are very rare tumors that originate from the sheath of schawnn, generally slow growing, and are usually asymptomatic. Treatment is surgical, often complex due to the anatomical location.The case of a 42-year-old female patient with a diagnosis of Schwannoma in the left parapharyngeal region, demonstrated by incisional biopsy, is presented; undergoing surgical treatment, which was carried out without complications.
Keywords: Parapharyngeal space; Schwannoma. (Source: MeSH Terms).
INTRODUCTION
Schwannomas are the second most frequent tumors located in the parapharyngeal space. Although most of these tumors are found in the head and neck, those with an extracranial location only constitute 10% of the total1. Parapharyngeal tumor lesions present a low incidence, representing between 0.5 and 0.8% of all head and neck tumors1,2. Approximately 80% show benign behavior2-4. The uniqueness of these lesions derives from their complex anatomical situation and the symptoms with which they usually appear, being in most cases nonspecific and almost always derived from the compressive effect produced by the lesion on the oropharynx and rhinopharynx, presenting symptoms such as dysphonia, compressive pain or pharyngeal mass.Secretory paraganglioma, although uncommon, can cause hypertension, sweating, nausea, palpitations or headache3These are usually tumors that affect adults, without differences between the sexes and are mostly benign.
The pathological study of the tumor reveals a well encapsulated mass made up of spindle cells type A of Anoni and type B of Antoni, the immunohistochemistry shows an intense expression of the S-100 protein5.
The prognosis for a person with schwannoma is excellent when the mass has been completely removed. Local recurrence is infrequent, being related to incomplete exegesis of the neoplasm6,7.
CLINICAL CASE
42-year-old female patient with a 20-year history of migraine. She presented to the Internal Medicine service of the Hospital Edgardo Rebagliati Martins in Lima, Peru, reporting a 2 months disease of progressive onset and characterized by hemicranial and left mandibular headache, of moderate intensity, accompanied by increased volume in the cervical region on the same side; also, mild odynophagia and dysphonia. Physical examination revealed a mass of approximately 5 cm in diameter in the left maxillary region, not adhered to deep planes, with non-hyperthermic surrounding skin and no color changes, nor fixed to deep planes, on bimanual manipulation it was discreetly painful on palpation. shallow and deep. Given the suspicion of an expansive parapharyngeal process, an imaging study was carried out using a Cervical Tomography with contrast (Figure 1), where a large solid left parapharyngeal mass with heterogeneous contrast enhancement and areas of peripheral calcification measured TD 38mm DL 50mm DBH 40mm , and that extends cranially towards the jugular foramen and displaces the cervical vascular structures anteriorly, without infiltration; causes mass effect with airway compression. In addition, a nuclear magnetic resonance study was performed (Figure 2,Figure 3), where it shows a solid image with well-defined edges, an ovoid shape in the left parapharyngeal space, exerting an expansive effect and moving the midline from left to right. Intramedullary extension is not observed. Subsequently, a BAAF was performed with ultrasound guidance of the lesion, the result of which was not conclusive for the diagnosis, which is why the case was reassessed, deciding to take an incisional biopsy by the Head and Neck Surgery Service, which was sent to histopathological study; Schwannoma was reported, being transferred for surgical treatment definitive; A cervical approach was used (Figure 4,Figure 5), and the surgical specimen was sent for histopathological study, the result of which confirmed our initial diagnosis: Parapharyngeal Schwannoma
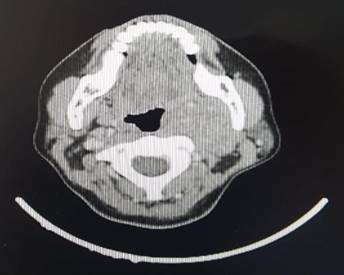
Figure 1: Contrast Tomography Scan of the neck, a large solid left parapharyngeal mass is evidenced with heterogeneous contrast enhancement and areas of peripheral calcification, measures DT 38mm DL 50mm DBH 40mm, which extends cranially towards the jugular foramen and displaces the cervical vascular structures anteriorly, without infiltration; causes mass effect with airway compression.
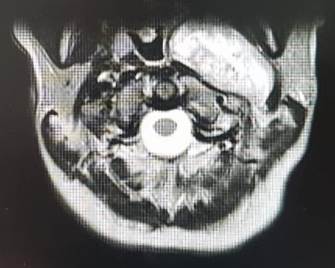
Figure 2A-2B: Magnetic Resonance Imaging of the neck with contrast, shows a solid image with well-defined edges, an ovoid shape in the left parapharyngeal space, exerting an occupational effect and shifting the midline from left to right. Intramedullary extension is not observed
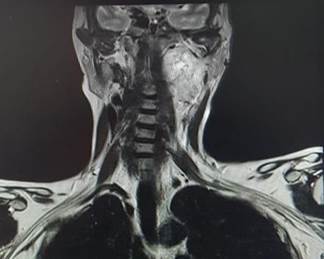
Figure 3A-3B: Taking an incisional biopsy, a cervical approach was used by the Head and Neck Surgery Service
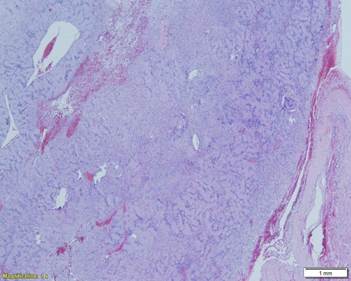
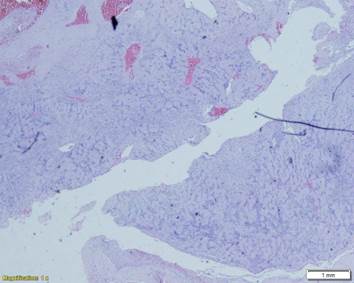
Figure 4: At lower magnification, a well-delimited and encapsulated tumor can be seen, and at this magnification the presence of palisade-shaped nuclei (Verocay bodies) can be seen
DISCUSSION
Parapharyngeal space tumors account for 0.5% of all head and neck neoplasms2. Most of the lesions located in this space are benign primary tumors that originate from the vagus nerve, the most common being the schwannoma. Schwannoma is the most common histologic subtype of vagus nerve tumor after paraganglioma. It usually appears between the third and sixth decades of life, being more frequent in young adults5, presenting a similar frequency in both sexes.3. Clinically without symptoms, it is diagnosed as a unilateral laterocervical mass mobile only in a solitary lateral direction, except in Von Recklinghausen's disease6,8and in a rare syndrome known as schwannomatosis(24)where the presentation is multiple. They can be palpated as masses on the medial border of the sternocleidomastoid muscle. Its expansive growth through the parapharyngeal space can make it go unnoticed to a large size. If its size is considerable, it can cause very nonspecific signs such as pharyngeal paresthesia, cough, odynophagia due to pharyngeal compression, dysphonia. A characteristic, although not always present, clinical sign of cervical vagal schwannoma is paroxysmal cough on palpation of the tumor and even serous otitis5,6,9. Symptoms derived from compression of nerve structures IX, X, XI, XII, of the sympathetic will be seen in cases of large neurinomas, or in malignant tumors and chemodectomas. Pain, trismus, and cranial nerve lesions suggest malignancy.
The diagnosis will be based on the clinic, the physical examination, being important the bimanual palpation, which allows to recognize the continuity of the tumor and determine its origin. Oropharyngeal and oral cavity visualization is important to rule out other primaries in these locations that could be producing secondary metastatic involvement in the parapharyngeal space. A pulsatile cervical mass may indicate the presence of a vascular tumor, such as a paraganglioma. The physical examination should include an examination of the cranial nerves and the performance of a flexible nasopharyngolaryngoscopy2.
The radiological study using Computed Tomography (CT) and Magnetic Resonance (MRI) will be of vital importance. On CT, they are tumors with a density similar to the muscle, more less rounded and well defined with a medial and lateral fatty plane, as their most frequent origin is the X pair or the sympathetic chain, they usually displace the internal carotid artery anteromedially. MRI provides excellent information in the study of soft tissues, being very useful in this type of tumors and that region,they are hypointense tumors on T1 and hyperintense on T2 and on T1 with gadolinium. Differential diagnosis should be made with carotid artery aneurysm, with neurogenic tumors of cranial nerves IX, X, XI and XII or of the cervical sympathetic plexus14, with paraganglioma, meningioma, lymphoma and teratoma15However, the majority of lesions involving the retrostyloid parapharyngeal space are peripheral nerve sheath tumors, head and neck paragangliomas, or metastatic lymphadenopathy(24).
The performance of FNAB in tumors of the pararaphinx can reach 86% - 99% especially in lymphoma, primary malignant tumors or metastases of malignant tumors(22,24). However, FNAB would not be helpful in distinguishing benign from malignant paragangliomas or benign from malignant peripheral nerve tumors. As in our case, it was not a contribution for diagnosis.
The macroscopic examination usually corresponds to a white, yellowish, well-defined mass with a firm and elastic consistency, sometimes with cystic areas. being typical the presence of necrosis, hemorrhage and intratumoral cystic degeneration(23). From the microscopic point of view there are two groups: Antoni A, a compact cellular composition in palisade and Antoni B, formed by a loose structure characterized by myxoid degeneration, although most of the time they are associated, while others defend that hemorrhage it is responsible for vacuolar degeneration due to hemosiderin deposition. Immunohistochemical techniques show an intense expression of the S-100 protein in these tumors, an antigen of the tissues derived from the neural crest (20, 21).
The treatment is surgical, although due to the infrequent presentation of tumors in this location it is difficult to obtain surgical experience, there are different approaches, which will depend on the size and location of the tumor, the most used being the cervical route, suitable for most tumors, in larger cases or for tumors of pre-style location, the cervico-parotid approach can be useful. The most frequent complications in surgery are injury to the nerve itself and its resulting deficit. Recurrences are rare and are usually the result of incomplete excision, generally having a good postsurgical prognosis. Regarding the prognosis, in cases of benign tumors, when a complete resection is achieved, the risk of recurrence should be low to null.
REFERENCES
1. Peter Pang K, Goh C, Ming Tan H. Parapharyngeal space tumours: an 18 year review. J Laryngol Otol 2002;116:170-5. [ Links ]
2. Olsen KD. Tumors and surgery of the parapharyngeal space. Laryngoscope 1994;104 (suppl 63). [ Links ]
3. Lawson VG, LeLiever WC, Makerewich LA. Unusual parapharyngeal lesions. J Otolaryngol 1979;8:241-9. [ Links ]
4. Andratschke M, Helmberguer R, Mess K. Differential diagnosis of parapharyngeal mass. Laryngorhinootologie 2000;79:174-9. [ Links ]
5. Asano K, Kubo O, Tajika Y, Ishii T, Tanikawa T, Kawamura H, et al. A clinico- pathological study of cystic spinal schwannomas. No To Shinkei 1996; 48: 245-51. [ Links ]
6. Donnelly MJ, Al-Sader MH, Blaney AW. View from beneath: Pathology in focus. Benign nasal schwannoma. J Laryngol Otol 1992; 106: 1011-5. [ Links ]
7. Nao EE, Dassonville O, Bozec A, Sudaka A, Marcy PY, Vincent N, et al. Cervical sympathetic chain schwannoma. Eur Ann Otorhinolaryngol Head Neck Dis 2012; 129: 51-3. [ Links ]
8. Najib Benmansour, Yasine Elfadl, Amal Bennani, Mustapha Maaroufi, Leila Chbani, Afaf Amarti, et al. Schwannome cervical du nerf vague: Stratégies diagnostique et thérapeutique. Pan Afr Med J 2013; 14: 76. [ Links ]
9. Chiofalo MG, Longo F, Marone U, Franco R, Petrillo A, Pezzullo L. Cervical vagal schwannoma. A case report. Acta Otorhinolaryngol Ital 2009; 29: 33-35. [ Links ]
10. De Araujo CE, Ramos DM, Moyses RA, Durazzo MD, Cernea CR, Ferraz AR. Neck nerve trunks schwannomas: clinical features and postoperative neurologic outcome. Laryngoscope 2008; 118: 1579-82. [ Links ]
11. Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O´Dwyer AJ, et al. Head and neck schwannomas - a 10-year review. J Laryngol Otol 2000; 114: 119-24. [ Links ]
12. Ríos A, Rodríguez JM, Febrero B, Parrilla P. Schwannoma extracraneal de origen simpático cervical. Rev Neurol 2012; 54: 638-9. [ Links ]
13. Gilmer-Hill HS, Kline DG. Neurogenic tumours of the cervical vagus nerve: report of four cases and review of the literature. Neurosurgery 2000; 46: 1498-503. [ Links ]
14. García-Marín A, Martín-Gil J, Bernardos-García LE, Gómez-Lanz L, Turégano- Fuentes F. Cervical cystic schwannoma of the vagus nerve. Cir Esp 2011; 89: 627- 8. [ Links ]
15. Varoquaux A, Fakhry N, Gabriel S, Garcia S, Ferretti A, Chondrogiannis S, et al. Retrostyloid parapharyngeal space tumors: a clinician and imaging perspective. Eur J Radiol 2013; 82: 773-82. [ Links ]
Received: July 19, 2021; Accepted: August 18, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
