










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.1 Lima ene./mar 2022 Epub 31-Dic-2021
http://dx.doi.org/10.25176/rfmh.v22i1.4123
Original article
Healthy lifestyle promotion and its effect on general practitioners at National Oncology Institute March - April 2021
1Instituto Oncológico Nacional de Panamá. Panamá.
2Unidad de Diabetes y Centro de Vida Sana “La Carlota”. Universidad de Montemorelos. Montemorelos, Nuevo León, México.
3Latin American Lifestyle Medicine Association. Lima, Perú.
Introduction:
The medical population is considered a representation of integral health. Its work characteristics predispose each member to be complicit in an unconscious practice and promotion of an unhealthy lifestyle. The aim of this work was to describe the effects on lifestyle of an educational intervention in general practitioners in an active work environment.
Methods:
This study included 18 general practitioners working at the “Instituto Oncológico Nacional de Panamá”. It consisted of 10 virtual educational sessions delivered by trained professionals for 2 months.
Results:
Positive changes and improvement in all measured variables were reported, including increased frequency of exercise sessions, increased duration of each session, increased consumption of fruits, vegetables, legumes and seeds, increased hours of sleep, improvement in the perceived stress scale score and a decrease in the consumption of foods with low nutritional quality.
Discussion:
Very little evidence exists regarding lifestyle promotion educational interventions aimed at health professionals. This population has a high predisposition to form a poor-quality lifestyle since the work environment in which the physician develops exposes him/her to adverse situations such as rotating schedules and long working hours with sleep deprivation.
Conclusions:
This practical and low-cost educational intervention achieved improvements in the lifestyle of physicians. For this reason, we recommend the replication of similar interventions and their documentation.
Keywords: Diet; Vegetarian; Lifestyle, Exercise, Nutritional Status. (Source : MeSH - NLM).
INTRODUCTION
The current pandemic due to Sars-Cov-2, exposes the vulnerability of patients with previously hidden chronic non-transmissible diseases, through the increase of risks of complications and mortality in case of infection by COVID-191. This phenomenon was identified early, strong evidence was published demonstrating that patients with hypertension, diabetes, cardiovascular diseases and chronic respiratory diseases have 3 times the risk of suffering from hospital complications secondary to COVID-192.
It is known that these chronic non-transmissible diseases have a direct relationship with habits and lifestyle3. The concept of lifestyle was described for the first time in 1979 by Alvin Toffler, writer and futurist, who predicted the explosion of different lifestyle forms of a postindustrial society. In modern times, lifestyle is considered a conscious or unconscious election of behavioral type which has a direct effect over the biological mechanisms that lead towards health or disease. These include changes in genetic expression, inflammation, oxidative stress, and metabolic dysfunction4.
In a lifestyle evaluation of health professionals, it was reported that only 11.5% of physicians practice a healthy lifestyle5. Taking into consideration these numbers we can deduce that approximately 9 out of 10 doctors practice habits unaligned with healthy lifestyle. Physicians and health professionals usually represent the the maximum authority in health matters and unconsciously communicate these poor habits to the general population. For this reason, it is of crucial importance to find effective and reproductive methods to improve the lifestyle of health professionals. The objective of this work is to provide information about the effects of educational intervention based on the promotion of a healthy lifestyle from the real working world.
METHODOLOGY
Design and area of study
A quasi-experimental study was performed, with pre and post educational intervention evaluations.
Population and sample
We invited general practitioners who worked in the Instituto Oncológico Nacional de Panamá to participate. A convenience sample was performed.
Variables and instruments
Data collection was carried out on 2 occasions, before initiating the intervention and after the same using the lifestyle evaluation from the American College of Lifestyle Medicine6as the instrument and the Spanish version of the Perceived Stress Scale7.
The Lifestyle Evaluation form is a scale by the American College of Lifestyle Medicine and Loma Linda University of Health which consists of 8 sections: General Health, Rest, Nutrition, Weight Control, Exercise, Purpose and Connection/Mental Health, Smoking/Drug use, and Motivation. With the objective of determining lifestyles and the possible risks of developing chronic diseases6.
The perceived Stress scale is an instrument which consists of 14 items that seek to evaluate life situations that are considered stressful. The actual version used for this study was validated for the Spanish language in a sample of 100 HIV+ patients. Through the evaluation of form and content we obtained a confidentiality determined by the Cronbach’s alpha coefficient value of 0.67. The answer options of the scale were Likert-type7.
Procedures
The intervention consisted of 10 educational sessions of 40 minutes in virtual modality These were presented by a team specialized in lifestyle behavioral changes, including physicians, psychologists, and nutritionists. The interventions were maintained for a lapse of 2 months, with a frequency of 2 sessions per week.
RESULTS
A total of 18 participants were included, the frequency of sex, ethnicity, smoking, alcoholism, schooling, and job shift were described in table 1. An age range between 28 and 45 years was reported, with an average and standard deviation of 38± 5,4 and 32± 6,2 years in women and men, respectively. The general average height was 168,2 ± 8,4 centimeters. (Table 1)
Table 1. General characteristics of the study participants
| Frequency | Percentage | Accumulated | |
| Age | |||
| Masculine | 32* | 6,2† | |
| Femenine | 38* | 5,4† | |
| Height | 168,2* | 8,4† | |
| Sex | |||
| Masculine | 10 | 55,55% | 55,55% |
| Femenine | 8 | 44,45% | 100,00% |
| Ethnicity | |||
| Mestizo | 12 | 66,66% | 66,66% |
| White | 2 | 11,11% | 77,77% |
| Hispanic-Asian | 1 | 5,55% | 83,32% |
| Black | 1 | 5,55% | 88,87% |
| Asian | 2 | 11,11% | 100,00% |
| Smoking | |||
| Smoker | 1 | 5,55% | 5,55% |
| Non-smoker | 17 | 94,45% | 100,00% |
| Alcoholism | |||
| Drink | 14 | 77,77% | 77,77% |
| Do not drink | 4 | 22,23% | 100,00% |
| Educational level | |||
| Licensed | 18 | 100,00% | 100,00% |
| Work shift | |||
| Rotate | 10 | 55,55% | 55,55% |
| Morning | 6 | 33,33% | 88,88% |
| Evening | 2 | 11,12% | 100,00% |
*Mean
†Standard Deviation
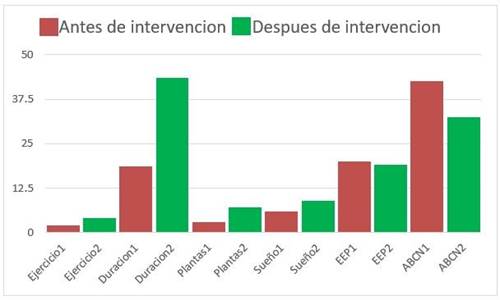
Positive changes and improvement are reported in all measured variables, these are exposed inFigure 1. The exercise sessions increased the average from 2 to 3 (33%) per week, the duration of each exercise session increased from 19 to 43 minutes (100%+), the daily portions of fruits, vegetables, legumes, and seeds increased from 4 to 6 (50%), the night sleep hours increased from 6 to 7 (16%), and there was improvement in the perceived stress scale score from 20 to 19 (5%0, furthermore a decrease in percentage of poor quality nutrition reported in the last 2 weeks was reported from 42% to 33% (22%). The most important change was shown in the duration of each exercise session.
DISCUSSION
The differences characteristic of lifestyle by geographic location have been described. The western countries tend to lean towards behaviors unaligned with healthy habits such as smoking, alcoholism, fat-rich diets, processed and ultra-processed foods, inactivity, and inadequate stress-management8. When everyday habits are not healthy, a substantial negative effect on health is added. The WHO has reported that people with an insufficient physical activity level have a death risk between 20% and 30% greater compared to people who reach a sufficient level of physical activity. Furthermore, the deficit in consumption of fruits, vegetables, seeds, and legumes is found in sixth place between risk factors of human mortality9.
On the other hand, the improvement and practice of healthy habits have a promising beneficial effect. The consumption of a balanced diet, rich in fruits and vegetables and enjoying physical activity on a regular basis is related to better competition of our immune and metabolic system. This results in less risk of chronic non-transmissible diseases and infectious diseases, a highly relevant benefit in our present10-12. It is estimated that 80% of cardiovascular diseases could be prevented by improving risk factors related to lifestyles13.
The lifestyle intervention and its metabolic benefits have been taken advantage in different parts of the world including developing countries due its low cost and feasibility14. In Nepal improvement on blood pressure has been reported in people with systemic arterial hypertension (SAH) and in adults without SAH15. Furthermore, significant benefits have been reported in all age ranges including preschool, elementary, high school students college students and housewives16-19.
Very little evidence exists in relation to educational interventions of lifestyle promotions directed to health professionals20. This population has a high predisposition to create a poor-quality lifestyle since the work environment in which the physician engages exposes them to adverse situations such as rotating schedule, long working days with sleep deprivation, emotional toll and high levels of stress21. It is necessary to consider health professionals as an important population for health promotion and chronic disease prevention programs. This, with the aim at improving health and establish them as model examples for their community, since physicians practice a healthy lifestyle have greater probability of recommending and inducing habits that are just as healthy in their patients22.
The educational intervention carried out in this study reached positive changes in the lifestyle of participants. An increase in the consumption of fruits and vegetables, increase in reported hours of sleep, a decrease in consumption of food of low nutritional quality, and increase in frequency of exercise sessions and duration of these were evidenced, being the latter the one which reported the most significant change. Regarding perceived stress, there was little improvement, we considered that diverse variables influence in the level in which the individual evaluates life situations such as stressors7. The data here presented orients a theory which, as the populations previously studied, general practitioners in the work environment are also sensitive to lifestyle educational interventions. The result in this case is a significant improvement in lifestyle. Additional studies are required in this population specifically with more intensive interventions, controlled and long term with the aim to identify more effective interventions for this population.
A weakness of this study was the short participant follow-up time, for this reason we propose a follow-up of 6 months and one year. We recommend carrying out similar interventions in the population of physicians and therefore reach positive changes in their health.
With a simple and low-cost educational intervention we were able to reach favorable changes in lifestyle of physicians.
REFERENCES
1. Serra Valdés MÁ. Las enfermedades crónicas no transmisibles y la pandemia por COVID-19. Rev Finlay. 2020;10(2):78-88. Disponible en: http://revfinlay.sld.cu/index.php/finlay/article/view/846 [ Links ]
2. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. 2020;94:91-5. DOI: https://doi.org/10.1016/j.ijid.2020.03.017 [ Links ]
3. De La Cruz Vargas JA, García García N, Sella L. Medicina de estilo de vida: El origen de una nueva especialidad médica. Rev Fac Med Humana. 2018;18(4):7-9. DOI: https://doi.org/10.25176/RFMH.v18.n4.1724 [ Links ]
4. Mora Ripoll R. Medicina del estilo de vida, la importancia de considerar todas las causas de la enfermedad. Rev Psiquiatr Salud Ment. 2012;5(1):48-52. DOI: https://doi.org/10.1016/j.rpsm.2011.04.002 [ Links ]
5. Diaz-Carrion EG, Failoc-Rojas VE. Estilos de vida en profesionales de salud de un hospital en Chiclayo, Perú 2017. Rev Habanera Cienc Médicas. 2020;19(5):1-10. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729-519X2020000600012 [ Links ]
6. Cramer T, Rea B. The Lifestyle Medicine Outpatient Clinic at Loma Linda University Health. Am J Lifestyle Med. 2018;12(5):425-7. DOI: https://doi.org/10.1177/1559827618766487 [ Links ]
7. Remor E, Carrobles JA. Versión Española de la Escala de Estrés Percibido (PSS-14): Estudio psicométrico en una muestra VIH+. Ansiedad Estrés. 2001;7(2-3):195-201. [ Links ]
8. Pastor Y, Balaguer I, García-Merita ML. Una revisión sobre las variables de Estilos de Vida Saludables. Rev Psicol Salud. 1998;10(1):15-52. DOI: https://doi.org/10.21134/pssa.v10i1.806 [ Links ]
9. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077-86. DOI: https://doi.org/10.1016/S2214-109X(18)30357-7 [ Links ]
10. Villagran Orellana M, Martínez Sanguinetti MA, Díaz F, Petermann-Rocha F, Celis-Morales C. Nutrientes, alimentación y actividad física como potenciadores del sistema inmune en tiempos de COVID-19.: Nutrients, diet, and physical activity as enhancers of the immune system in times of COVID-19. ARS MEDICA Rev Cienc Médicas. 2020;45(4):48-60. DOI: https://doi.org/10.11565/arsmed.v45i4.1732 [ Links ]
11. World Health Organization. Regional Office for Europe. Development of a WHO global strategy on diet, physical activity and health : European regional consultation : report on the Consultation, Copenhagen, 2-4 April 2003 [Internet]. Copenhagen: WHO Regional Office for Europe; 2003 [citado 2 de noviembre de 2021]. Report No.: EUR/03/905732HQ. Disponible en: https://apps.who.int/iris/handle/10665/107508 [ Links ]
12. Guerrero Barona EJ. Salud, estrés y factores psicológicos. Campo Abierto Rev Educ. 1996;(13):49-70. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=118970 [ Links ]
13. World Health Organization. Office of World Health Reporting. The World health report : 2002 : reducing risks, promoting healthy life : overview [Internet]. World Health Organization; 2002 [citado 2 de noviembre de 2021]. Report No.: WHO/WHR/02.1. Disponible en: https://apps.who.int/iris/handle/10665/67454 [ Links ]
14. Quillas Benites RK, Vásquez Valencia C, Cuba Fuentes MS. Promoción de cambios de comportamiento hacia estilos de vida saludable en la consulta ambulatoria. Acta Médica Peru. 2017;34(2):126-31. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1728-59172017000200008 [ Links ]
15. Neupane D, McLachlan CS, Mishra SR, Olsen MH, Perry HB, Karki A, et al. Effectiveness of a lifestyle intervention led by female community health volunteers versus usual care in blood pressure reduction (COBIN): an open-label, cluster-randomised trial. Lancet Glob Health. 2018;6(1):e66-73. DOI: https://doi.org/10.1016/S2214-109X(17)30411-4 [ Links ]
16. Carranza Esteban RF, Caycho-Rodríguez T, Salinas Arias SA, Ramírez Guerra RM, Campos Vilchez C, Chuquista Orci K, et al. Efectividad de intervención basada en modelo de Nola Pender en promoción de estilos de vida saludables de universitarios peruanos. Rev Cuba Enferm. 2019;35(4):1-10. Disponible en: http://www.revenfermeria.sld.cu/index.php/enf/article/view/2859/500 [ Links ]
17. Fretes G, Salinas J, Vio F. Efecto de una intervención educativa sobre el consumo de frutas, verduras y pescado en familias de niños preescolares y escolares. Arch Latinoam Nutr. 2013;63(1):37-45. Disponible en: http://ve.scielo.org/scielo.php?pid=S0004-06222013000100005&script=sci_abstract [ Links ]
18. Veramiendi N. Intervención de estrategias de enseñanza en estilos de vida saludables de las amas de casa, localidad de Pillcomarca-Huánuco 2012. Rev Educ Desarro Soc. 2013;7(1):63-70. DOI: https://doi.org/10.18359/reds.734 [ Links ]
19. Elizondo-Montemayor L, Gutiérrez NG, Sánchez DMM, Monsiváis Rodríguez FV, Martínez U, Nieblas B, et al. Intervención para promover hábitos saludables y reducir obesidad en adolescentes de preparatoria. Estud Soc Rev Aliment Contemp Desarro Reg. 2014;22(43):217-39. Disponible en: https://www.redalyc.org/articulo.oa?id=41729386009 [ Links ]
20. Menor Rodríguez M, Aguilar Cordero M, Mur Villar N, Santana Mur C. Efectividad de las intervenciones educativas para la atención de la salud: Revisión sistemática. MediSur. 2017;15(1):71-84. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1727-897X2017000100011 [ Links ]
21. Mingote Adán JC, Moreno Jiménez B, Gálvez Herrer M. Desgaste profesional y salud de los profesionales médicos: revisión y propuestas de prevención. Med Clínica. 2004;123(7):265-70. DOI: https://doi.org/10.1016/S0025-7753(04)74484-X [ Links ]
22. Frank E, Rothenberg R, Lewis C, Belodoff BF. Correlates of physicians' prevention-related practices. Findings from the Women Physicians' Health Study. Arch Fam Med. 2000;9(4):359-67. DOI: https://doi.org/10.1001/archfami.9.4.359 [ Links ]
Received: August 16, 2021; Accepted: December 07, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
