










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.1 Lima ene./mar 2022 Epub 31-Dic-2021
http://dx.doi.org/10.25176/rfmh.v22i1.4339
Original article
Clinical profile of patients before and after a diabetes reversal program in Ecuador
1Centros Médicos Dr. Marco Albuja. Quito, Ecuador.
2Universidad Internacional del Ecuador. Quito, Ecuador.
Introduction:
Chronic non-communicable diseases (NCDs) are the main cause of death in Ecuador and the world, and within them diabetes mellitus is one of the fastest growing morbidity and mortality.
Objective:
To determine if there are differences between the clinical characteristics before and after a diabetes reversal program in Ecuador.
Methods:
Comparative study before and after in the same individual. Patients who voluntarily entered an outpatient clinical program based on Lifestyle Medicine were followed for 8 weeks, measures were taken at the beginning and at the end of this period, which included plant-based nutrition, physical exercise and psychological support.
Results:
Eight patients were analyzed between 40 and 74 years (3 women and 5 men) The comparative analysis before and after the intervention showed significant differences for: Weight (p = 0.007), BMI (p: 0.004), Glucose (p = 0, 04), glycosylated hemoglobin (p = 0.007), triglycerides (p = 0.04), urea (p = 0.004), and TGP (p = 0.023).
Conclusions:
There is an improvement in the variables measured after having carried out the “Lifestyle Medicine” reversal program compared to the initial measurements.
Keywords: Life Style; Health Behavior; Health (Source: MeSH NLM).
INTRODUCTION
Chronic noncommunicable diseases are the leading cause of death and disease in the world1. In Ecuador the situation is no different, according to the results of the STEPS survey on noncommunicable diseases and risk factors, conducted in 2018 to people between 18 and 69 years old, it was obtained that the percentage of people with overweight and obesity is 63.6% (95% CI: 61.8 - 65.4), of these the percentage of people with obesity reaches 25.7% (95% CI: 24.1 - 27.3), with respect to diabetes mellitus, the percentage of people with impaired fasting blood glucose (between 110 and 126 mg/dl) is 7.8% (95% CI: 6.8 - 8.9), of these the percentage of people with elevated fasting blood glucose (greater than 126 mg/dl) reaches 7.1% (95% CI: 6.1 - 8.1)2.
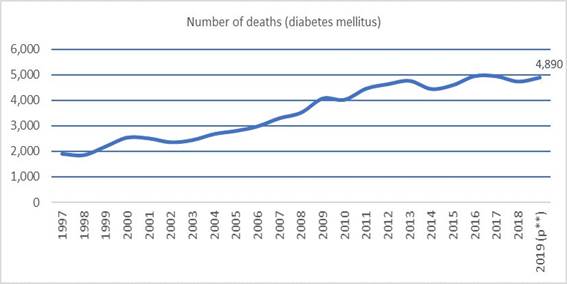
Diabetes mellitus was the second leading cause of death in Ecuador in 2019, being directly responsible for 4,890 deaths3. The participation of this pathology in deaths in Ecuador has grown steadily and considerably in recent years (Figure 1), and may contain a significant underreporting since it is not always identified as the underlying cause of death, so the figure could be even higher.
There are abundant references worldwide that show that lifestyle medicine is effective in improving blood glucose levels in chronic patients with diabetes mellitus, often leading to the reversal of prediabetes or diabetes4-6. Currently in Ecuador there is not much offer of reversal programs for chronic noncommunicable diseases, being the plan de Medicina de Estilo de Vida (MEV) of Dr. Marco Albuja, the pioneer reversal program of this type in the country, which consists of eight weeks of transition to a new lifestyle that includes plant-based diet, physical exercise, psychological support and constant clinical monitoring, and a subsequent monitoring of health conditions for at least one year.
Therefore, the objective of the present study is to determine if there are differences between the clinical characteristics before and after a diabetes reversal program in Ecuador.
METHODS
Design and study area
Longitudinal, comparative study of outpatient intervention in Lifestyle Medicine, carried out in Quito - Ecuador, parameters were evaluated before and after the intervention.
Population and sample
The reference population was the patients who voluntarily entered the Lifestyle Medicine program at the Medical Center in Quito, Ecuador. The study consisted of comparing 8 patients (sample size, n = 8) who entered the "Lifestyle Medicine" reversal program on different dates. The selection of individuals for the study was done by convenience sampling. This indicates that this study does not seek to extrapolate its results to the general population but seeks to describe the results for this particular set of 8 selected patients7.
Variables and instruments
Laboratory samples were taken at baseline and at the end of the program, and the following indicators were measured: Weight (in kilograms), Body Mass Index, basal glucose (mg/dl), basal hemoglobin (mg/dl), basal glycosylated (mg/dl), uric acid (mg/dl), quantitative microalbuminuria (mg/dl), cholesterol (mg/dl), HDL (mg/dl), LDL (mg/dl), triglycerides (mg/dl), TSH (mU/L), creatinine (mg/dl), urea (mg/dl), TGO (mg/dl) and TGP (mg/dl).
Procedures
All 8 patients underwent the outpatient lifestyle medicine intervention consisting of an 8-week program of the stop-and-reverse plan for chronic disease, which included a comprehensive approach of plant-based nutrition, scheduled physical activity, psychological and spiritual support. The program was administered by a team of physicians, nutritionists, psychologists and a physical trainer.
Patients who are candidates for the MEV program undergo an initial consultation where they are given a general explanation of what the program consists of. If they decide to enter the program, initial examinations are scheduled, which include imaging and blood tests and an initial evaluation in five specialties: nutrition, psychology, cardiology, endocrinology and sports medicine. The eight weeks of the reversal program begin with an inauguration event where operational information is given about the follow-up of the process, which is done in person and in groups using Whatsapp, in which patients must report all food consumed and exercise performed, which is followed and individually fed back by the nutritionist and physical trainer. On a weekly basis, the entire medical and follow-up team evaluates the evolution of each patient in the group, and in these team meetings clinical decisions are made, such as reduction or increase of medications, diet and intensity of physical exercise, among others.
At the end of the 8 weeks, the same series of laboratory tests that were done at the beginning of the program are performed again to evaluate the results in each of the selected patients. The first phase of the program ends with a closing session where the results are shown to all patients and the subsequent follow-up of health conditions is coordinated and monitored if the transition to the new lifestyle is maintained over time.
The COVID-19 pandemic implied certain operational modifications in the MEV program process, since it became impossible to hold the meetings for physical exercise outdoors, the start and end meetings were virtual, but although it is true that technology was used to continue with the program, the conceptual essence of the program did not suffer important modifications.
The 8 patients selected in this study do not belong to a single group of patients, but to several groups over time in order to better capture the variability between various groups of patients and avoid selection bias of a single group with particular conditions, some patients were in groups before the pandemic, and others in groups during the pandemic, which has not yet ended in Ecuador and the world (at the date of publication of this article).
Statistical analysis
To compare the results before and after the program, parametric (paired t-test or for related samples) and nonparametric (Wilcoxon test for paired or related samples) statistical tests were used because of the sample size. All hypothesis tests were performed at a significance level of 5% and tests were performed to assess normality (Shapiro-Wilks test). In the absence of sufficient evidence of normality of the data, the Wilcoxon test was chosen.
RESULTS
The final sample of the study was 8 patients,Table 1describes the characteristics of weight and biochemical tests taken before and after the program, variations are observed in all variables, such as decrease in weight (from 86.3 kg to 77.2 kg), decrease in glucose (from 143, 3 mg/dL to 102.28 mg/dL), in the case of lipids we found a decrease in cholesterol (from 209.9 mg/dL to 186.8 mg/dL) and LDL (from 134.1 mg/dL to 113.5 mg/dL), increase in HDL (from 43.6 to 47.5 mg/dl), a decrease in transaminases, as well as creatinine and urea.
Table 1. General characteristics before and after the intervention in the lifestyles of the population studied.
| Variable | Before the intervention | After the intervention | ||||||
| Minimum | Median | Medium | Maximum | Minimum | Median | Medium | Maximum | |
| Weight | 48 | 85,7 | 86,3 | 134 | 45 | 78,5 | 77,2 | 114 |
| IMC | 22,5 | 31,7 | 32 | 42,2 | 21,1 | 28,0 | 28,6 | 35,5 |
| Glucose | 96 | 124,9 | 143,6 | 285 | 81,7 | 102,3 | 102,2 | 138 |
| HBAIC | 5,5 | 6,6 | 7,6 | 12,0 | 4,7 | 5,4 | 5,7 | 7,9 |
| Uric acid | 3,4 | 6,5 | 6,22 | 7,9 | 4,8 | 5,5 | 6,2 | 9,8 |
| Microalbuminuria | 3 | 6,4 | 65,7 | 417 | 3,0 | 4,9 | 63,7 | 449 |
| Cholesterol | 170 | 191 | 209,9 | 266 | 138,2 | 191,5 | 186,8 | 241 |
| HDL | 30,6 | 42,5 | 43,6 | 57 | 33,5 | 46 | 47,4 | 69,3 |
| LDL | 107 | 129,9 | 134,1 | 169 | 85,8 | 113,8 | 113,5 | 158 |
| Triglyceride | 94 | 130,5 | 144,1 | 246 | 58,5 | 100 | 108,3 | 162 |
| TSH | 0,7 | 1,7 | 2,6 | 6,8 | 1,21 | 1,87 | 2,9 | 9,6 |
| Creatinine | 0,6 | 0,9 | 0,9 | 1,6 | 0,5 | 0,835 | 0,8 | 1,05 |
| Urea | 28 | 34,5 | 38,0 | 66,4 | 15,7 | 20,85 | 22,2 | 32,9 |
| TGO | 18 | 26 | 29,5 | 47 | 16,1 | 25,4 | 25,3 | 36 |
| TGP | 20 | 31 | 42,3 | 84,4 | 13,6 | 22,9 | 24,5 | 37,2 |
Intabla 2we found that the variable glucose, uric acid, microalbuminuria, TSH and urea do not follow a normal distribution unlike the other variables.
Table 2. Normality tests
| Variable | p-value for Shapiro-Wilks test (Before) | p-value Shapiro-Wilks test (After) |
| Weight | 0,651 | 0,544 |
| IMC | 0,604 | 0,897 |
| Glucose | 0,006* | 0,317 |
| HBAIC | 0,144 | 0,090 |
| Uric acid | 0,091 | 0,029* |
| Microalbuminuria | <0,001* | <0,001* |
| Cholesterol | 0,081 | 0,894 |
| HDL | 0,795 | 0,654 |
| LDL | 0,577 | 0,378 |
| Triglyceride | 0,172 | 0,299 |
| TSH | 0,0123* | 0,001* |
| Creatinine | 0,239 | 0,616 |
| Urea | 0,007* | 0,424 |
| TGO | 0,256 | 0,915 |
| TGP | 0,221 | 0,343 |
*p<0,05
Tabla 3shows the p-values according to the statistical tests performed to compare the values of the variables measured before and after the intervention program.
Table 3. P-values of statistical tests
| Variable | p-value of one-tailed t-test | One-tailed Wilcoxon test p-value |
| Weight | 0,001* | 0,007* |
| IMC | <0,001* | 0,003* |
| Glucose | 0,050 | 0,039* |
| HBAIC | 0,028* | 0,007* |
| Uric acid | 0,51 | 0,578 |
| Microalbuminuria | 0,831 | 0,710 |
| Cholesterol | 0,101 | 0,125 |
| HDL | 0,151 | 0,191 |
| LDL | 0,085 | 0,074 |
| Triglyceride | 0,039* | 0,039* |
| TSH | 0,648 | 0,578 |
| Creatinine | 0,187 | 0,444 |
| Urea | 0,003* | 0,003* |
| TGO | 0,150 | 0,148 |
| TGP | 0,022* | 0,023* |
*p<0,05
DISCUSSION
The results show that the reversal program "Lifestyle Medicine" significantly improves in 8 weeks the indicators related to the pathology of diabetes mellitus in the 8 patients analyzed, such as weight and glucose in which a significant reduction in the level of the variable is observed, and others in which the reduction is less; A similar result was found in a longitudinal study conducted in women, where a significant improvement in anthropometric measures (weight, BMI, body fat, lean mass) was obtained, but no comprehensive intervention was performed on the participants, so no metabolic data were collected, where similar results to our study could possibly be found8.
Likewise, most of the variables follow a normal distribution, with the exception of glucose, uric acid, microalbuminuria, TSH and urea. After performing normality tests, it is concluded that the following variables improved significantly after the "Lifestyle Medicine" reversal program: Weight, BMI, glucose, glycosylated hemoglobin, triglycerides, urea and TGP, this means that the implementation of lifestyle change programs are adequate to reduce the morbimortality of non-communicable diseases, such as diabetes mellitus, as well as to decrease its incidence, in addition these programs must have an adequate support team for the integral follow-up of the person, as pointed out in a longitudinal study conducted in adolescents with overweight or obesity, although they did not find significant results in all metabolic variables, such as cholesterol and uric acid levels, good results were obtained in the anthropometric variables9, as well as in a review study10which indicates that carrying out lifestyle interventions at an early age has positive long-term effects, such as greater awareness and basic knowledge on the subject, thus reducing the risk of non-communicable diseases in adulthood.
Among the limitations of the study we have the size of the sample and its selection, remember that the results obtained in this article are particular to the 8 individuals analyzed, and in order to extrapolate these results to a larger reference population it would be necessary to choose subjects at random using probability sampling techniques, choosing people of different ages, socioeconomic strata, gender, among others. This becomes difficult because it would imply having a source of funding so that the availability of economic resources does not generate a sample selection bias, in this study and in the MEV program analyzed, patients self-finance their participation.
Since there are few cases in this study, the statistical tests require a greater difference to be able to establish that this is statistically significant; the sample size may also be hiding the fact that other dimensions may show improvement in their levels, but this is not large enough to be considered significant given the greater standard error of the sample mean.
CONCLUSION
In conclusion, there is an improvement in some variables measured after taking the "Lifestyle Medicine" reversal program compared to baseline measures in the 8 patients monitored for 8 weeks. These were weight, BMI, glucose, glycosylated hemoglobin, triglycerides, urea and TGP. An intervention with more patients is recommended in order to improve the statistical significance of the tests and to have more robust conclusions that can be extrapolated to the general population
REFERENCES
1. World Health Organization. STEPwise approach to surveillance (STEPS). [Online] Teams WHO. 2021 [cited 2020 Mayo 20]. Available from: https://www.who.int/ncds/surveillance/steps/en/. [ Links ]
2. Ecuador MdSd. Vigilancia de enfermedades no transmisibles y factores de riesgo. Informe de resultados. [Online]. 2018 [cited 2020 Mayo 20]. Available from: https://www.salud.gob.ec/wp-content/uploads/2020/10/INFORME-STEPS.pdf [ Links ]
3. Instituto nacional de estadística y censos. Defunciones generales. [Online]. INEC. 2020 [cited 2020 Mayo 20]. Available from: https://www.ecuadorencifras.gob.ec/defunciones-generales-2019/. [ Links ]
4. Garry Egger ABSRMS. Medicina del estilo de vida: Hábitos, entorno, prevención y promoción de la salud. 3rd ed. Elsevier; 2017. [ Links ]
5. ACPM. Lifestyle medicine resources. [Online]. 2021 [cited 2020 Mayo 20]. Available from: https://www.acpm.org/initiatives/lifestyle-medicine/lifestyle-medicine-resources/. [ Links ]
6. De La Cruz J, Dyzinger W, Herzog S,Dos Dantos F, Villegas H, Ezinga M. Medicina del Estilo de Vida: Trabajando juntos para revertir la epidemia de las enfermedades crónicas en Latinoamérica. Ciencia e Innovación en Salud. 2017; 4(2):1-7. DOI: https://doi.org/10.17081/innosa.4.2.2870 [ Links ]
7. Torres E, Arévalo H, Suárez I, Vega N. Perfil clínico de pacientes atendidos con Diabetes Mellitus tipo 2 en un programa de reversión. Rev Fac Med Hum. 2021; 21(1):124-129. DOI: http://dx.doi.org/10.25176/rfmh.v21i1.3432 [ Links ]
8. Fernández-García JC, Gálvez-Fernández I, Gavala-Gonzáles J. Estudio longitudinal sobre la pérdida de peso en mujeres jóvenes. J Sport Health Res. 2019; 11(1): 105-114. Available from: https://recyt.fecyt.es/index.php/JSHR/article/view/80936 [ Links ]
9. Ortega A. Efecto en la modificación de los estilos de vida en adolescentes de 10 a 14 años con obesidad de la unidad de medicina familiar número 2. [Tesis de especialidad]. Puebla, México: Universidad Autónoma de Puebla, 2019. Available from: https://repositorioinstitucional.buap.mx/handle/20.500.12371/11310 [ Links ]
10. Pardos-Mainer E, Gou-Forcada B, Sagarra-Romero L, Calero S, Fernádez RR. Obesidad, intervención escolar, actividad física u estilos de vida saludable en niños españoles. Rev Cubana Salud Pública. 2021; 47(2). Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34662021000200017 [ Links ]
Received: October 26, 2021; Accepted: December 07, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
