










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.1 Lima Jan./Mar. 2022 Epub Dec 31, 2021
http://dx.doi.org/10.25176/rfmh.v22i1.4137
Clinical case
Diabetic foot and lifestyle: Case report
1Hospital Nacional Dos de Mayo
Introduction:
Diabetes is still the leading cause of non-traumatic amputation in most Western countries, epidemiological reports indicate that more than a million amputations are performed in people with diabetes each year, this is equivalent to an amputation for diabetes somewhere in the world every 30 seconds, most of these amputations are preceded by ulcers.
Clinical Case:
We present a case of a 39-year-old male patient suffering from diabetes mellitus and uncontrolled hypertension, with late complications, chronic kidney disease, anemia, retinopathy, and ischemic and neuropathic diabetic foot, with indication for amputation. Healthy lifestyles are used, controlling glycemia, hypertension, without requiring medication and reducing proteinuria. There were no adverse effects. With favorable evolution since then.
Conclusion:
A healthy lifestyle is an intervention that the earlier it is used, the greater its benefits, without the risk of adverse effects or unnecessary costs, but even in late stages it has shown benefits in glycemic, hypertensive and renal control.
Keywords: Diabetic foot; Life style; Diabetic Nephropathy.(fuente: MeSH NLM).
INTRODUCTION
Diabetes remains the leading cause of non-traumatic amputation in most Western countries, rates are up to 15 times higher than in the non-diabetic population1, epidemiological reports indicate that over one million amputations are performed in people with diabetes each year, this equates to one diabetic amputation somewhere in the world every 30 seconds, most of these amputations are preceded by ulcers. Only two-thirds of ulcers heal over time and the remainder may result in some form of amputation, with the average healing time for an ulcer being approximately six months. Both ulcers and amputations have a huge impact on people's lives, and often lead to dependency, social isolation and psychological stress2.
PATIENT INFORMATION
Male patient, 39 years old, native from Lima, with a history of diabetes mellitus since he was 8 years old, obesity since then with BMI >40, until 10 years ago when he started to lose weight and reached a BMI 22, on treatment with Glibenclamide until 10 years ago when she started with insulin NPH 20U and metformin 850mg since 10 years ago, Arterial Hypertension 10 years ago on treatment with Nifedipine 30mg c/24h, Losartan 50mg c/12h, amputation of the 1st toe of the right foot 01/2020.
Family History: Mother, 2 sisters and maternal grandfather with diabetes mellitus.
Patient had been ill for 4 days before admission and noticed two ulcers, one in the previous surgical site and others in the plantar region, associated with foul odor and purulent discharge.
During his hospitalization the patient presents with glycemia > 400 predominantly post prandial, with indication for supracondylar amputation by medical board with the specialties of cardiovascular surgery, traumatology and internal medicine.
CLINICAL FINDINGS
PA:140/70, FC 72, FC: 62, FR 19, Sat O2: 98
Weight: 72, Height: 1.75, IMC: 22
There is evidence of hyperpigmentation of the skin, cavus foot, claw toes, widening with bony prominences in the plantar region and in the internal and external borders, ulcer at the base of the 1st metatarsal in the bed of previous surgery of 3*4cm, plantar ulcer of 3*2cm, at the base of the 3rd metatarsal with necrotic tissue, purulent secretion, bad odor, erythema, heat, edema, pain in the surrounding skin.
Decreased pedial pulses.
Fundus: Severe proliferative diabetic retinopathy in both eyes, retinal detachment.
ECODOPPLER: Mild bilateral atherothrombosis in bilateral femoral and popliteal arteries, severe atherothrombosis with diffuse lesions in infrapopliteal arteries between 50-75%.

Figure 1: Cavus foot, with claw toes, ulcer at the base of the first metatarsal, with necrosis, edema, perilesional

DIAGNOSIS
-Diabetic Foot Pedis III - Neuropathic and Ischemic
-Uncontrolled Type 2 Diabetes Mellitus With Late Complications
Non Proliferative Diabetic Retinopathy
Diabetic Polyneuropathy
Peripheral Arterial Insufficiency
Chronic Kidney Disease: Diabetic Nephropathy G4 A3
-Uncontrolled Arterial Hypertension
-Mild Multifactorial Anemia.
THERAPEUTIC INTERVENTION
Air: Breathing exercises, where deep thoracoabdominal breathing is strengthened, at least 10 times a day.
Rest: Sleep 7-8 hours, no later than 10pm.
Exercise: Given his condition of diabetic neuropathic foot, complicated with plantar ulcer, patient conditioned orthopedic boot, with which he exercised about 1 hour daily (bicycle) to go to work, as his means of transportation, as well as with weights (created by him) 2 times a week, especially for strengthening the upper limbs.
Food: Diet with a predominance of plants, white flour, simple sugars, fried foods, and encouraged the consumption of whole foods, vegetable proteins, polyunsaturated fats (low cost seeds, olives), omega 3 (flaxseed), fiber, salt intake was reduced, especially by avoiding the consumption of processed foods.
Water: 2 liters of water per day, maintain neutral balance.
Temperance: Avoid food between meals, no tobacco, no alcohol, no sugar.
Sunlight: 30 minutes of sun exposure
Trust in God: Daily time for meditation.
Daily healing of the foot: Water with activated charcoal for 14 minutes was prepared, then the foot was cleaned with soap and water to remove the devitalized tissue.
Family time was encouraged: The economic circumstances, added to the pandemic, isolated the family, therefore community life was encouraged, especially scheduling family visits.
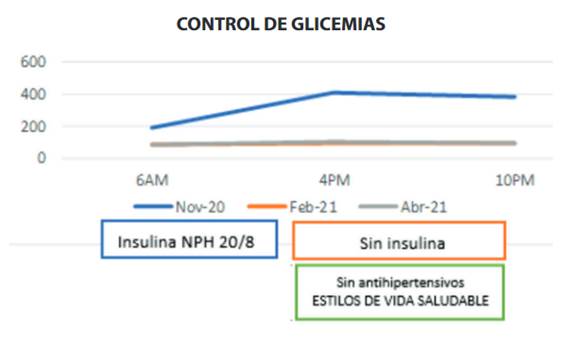
Table 1. Laboratory Test Trends
| EXAMEN | 11/2020 | 02/2021 | 04/2021 |
| GLICEMIAS PREPRANDIALES | 170-200 | 140 | 100 |
| GLICEMIAS POSTPRANDIALES | 200-400 | ||
| HEMOGLOBINA GLICOSILADA | 10.7 | ||
| CREATININA | 3.26 | 2.37 | |
| UREA | 96.91 | 97 | |
| HB/HTO | 8.7/25.6 | 10.9/31.5 | |
| TRIGLICERIDOS | 184 | 48 | |
| COLESTEROL TOTAL | 204 | 249 | |
| HDL | 41 | 87 | |
| LDL | 127 | 153 | |
| PROTEINURIA DE 24H | 4.25 | 3.066 | |
| DEPURACIÓN DE CREATININA | 47.3 | ||
| VITAMINA B12 | 768 | 542 |
Patient remains adhered to the treatment with 1 monthly follow-up, in person or by telephone, with supervision by means of photos of the food eaten, as well as of the glycemia in real time glucometer, at the beginning of treatment he presented a decrease in glycemia, without reaching symptomatic hypoglycemia, due to close control of the same, which was leveled in 2 weeks, managing to withdraw the insulin, as well as suspending the antihypertensive drugs.
Likewise, improvement of the described ulcers was evidenced.

Figura 4: 1cm scar, no discharge, no edema, no surrounding erythema, plantar lesion completely resolved
Patient tolerated the indicated treatment, especially in the items of food, exercise, temperance, with adequate adherence, presenting glycemic control 2 weeks after discharge, without medication, as well as blood pressure control.
DISCUSSION
Diabetes remains the leading cause of non-traumatic amputation in most Western countries, rates are up to 15 times higher than in the non-diabetic population1, epidemiological reports indicate that more than one million amputations are performed in people with diabetes each year, this is equivalent to an amputation due to diabetes somewhere in the world every 30 seconds, most of these amputations are preceded by ulcers. Both ulcers and amputations have a huge impact on people's lives, and often lead to dependency, social isolation and psychological stress2. It was the therapeutic decision to amputate that led to a lifestyle change in our patient.
Diabetes is a preventable disease, as we saw in our patient suffered from obesity from an early age, as well as the family environment, which supports an important genetic load, which unfortunately shows that a late intervention in a person, no matter how young, leaves severe damage in multiple organs, however even being a late intervention it has been possible to objectify the positive impact, not only avoiding amputation, but keeping him economically active, not limiting his mobilization or economic expenses due to the disease itself.
Persistently elevated glucose has contributed unfavorably in the damage to multiple organs, such as the torpid evolution of ulcers, as well as arterial hypertension3.
Taking as a principle a DASH diet3with a predominance of plant consumption, added to reduced sodium consumption4, especially by limiting processed foods, adequate fluid intake, these changes have had a benefit in glycemic, hypertensive6and renal control, presenting no complications of the internal environment despite renal compromise, improving hemoglobin values, which encourages the plant-based diet, not only for its benefit in diabetes and hypertension but in renal patients, breaking old myths.
Exercise benefits not only at the cardiovascular level, but also by increasing insulin sensitivity7.
Adequate rest5has reduced the consumption of harmful foods and insulin resistance; however, adherence was limited by the socio-economic context, which reduced the hours and quality of sleep, not calling into question its benefits, but encouraging greater emphasis on the emotional and spiritual aspect, which, as expressed by the WHO, has an undoubtedly positive impact on health.
No adverse effects were found that limit a healthy lifestyle even in advanced stages of the disease, but it does encourage the need for education and early interventions, which will improve quality of life, reduce health expenses, avoid complications and improve survival.
One of the challenges was the isolation during the pandemic, limiting face-to-face evaluations, especially for support in healing, so more interest was placed on patient and family education, as well as using less expensive healthy foods, exercise became part of their daily routine, which did not overload their daily work, finding a sport that is also their means of transportation.
Multidisciplinary management is necessary in these patients, given that it is a disease with multiple complications, devising new strategies, especially in this type of context should be our goal so that more patients are reached, despite the pandemic and economic limitations.
CONCLUSIONS
Healthy lifestyle is an intervention that the earlier it is employed the greater the benefits, without the risk of adverse effects or unnecessary costs, but even in late stages it has shown benefits in glycemic, hypertensive and renal control.
The limitation in lipid control was influenced by renal compromise, as the patient presented nephrotic syndrome.
REFERENCES
1. Dan Ziegler. Painful diabetic neuropathy: treatment and future aspects Diabetes Metab Res Rev 2008;24(Suppl 1): S52-S57. [ Links ]
2. Guía De Practica Clínica De Prevención Y Manejo Del Pie Diabético Como Complicación De La Diabetes Mellitus. Hospital Almenara. Lima-Perú 2013 [ Links ]
3. Asociación Americana de Diabetes. Diabetes Care 2021 Jan; 44 (Suplemento 1): S151 -S167.https://doi.org/10.2337/dc21-S011 [ Links ]
4. Andrea Grillo, Lucia Salvi, Paolo Coruzzi, Paolo Salvi, and Gianfranco Parati. Sodium Intake and Hypertension. Nutrients 2019, 11, 1970. [ Links ]
5. Katri Peuhkuri , Nora Sihvola , Riitta Korpela. Diet promotes sleep duration and quality. Nutr Res. 2012 Mayo; 32 (5): 309-19. [ Links ]
6. Pedro L. Valenzuela, Pedro Carrera-Bastos, Beatriz G. Gálvez, Gema Ruiz-Hurtado, José M. Ordovas, Luis M. Ruilope yAlejandro Lucía. Lifestyle interventions for the prevention and treatment of hypertension. 18, pages251-275(2021). Nature Reviews Cardiology.2020. [ Links ]
7. Influence of Physical Activity on Hypertension and Cardiac Structure and Function. Sheila M. Hegde and Scott D. Solomon. Cardiovascular Division, Brigham and Women's Hospital, Harvard Medical School, Boston, MA. Curr Hypertens Rep. 2015 Oct;17(10):77. [ Links ]
Received: September 24, 2021; Accepted: November 02, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
