










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.2 Lima abr./jun 2022 Epub 16-Mar-2022
http://dx.doi.org/10.25176/rfmh.v22i2.4792
Clinical case
Tuberculosis orchiepididymitus in insulin-dependent type 2 diabetes mellitus: Case report
1Facultad de Medicina Humana, Universidad Peruana Los Andes. Huancayo, Perú.
2Sociedad Científica de Estudiantes de Medicina Los Andes (SOCIEMLA). Huancayo-Perú.
3Hospital Nacional “Ramiro Prialé Prialé” R.A.J. Huancayo-Perú.
Introduction:
Peru has little information about the association of tuberculous orchiepididymitis in relation to immunosuppressed patients, being a country endemic for tuberculosis and having an increased prevalence of chronic non-communicable diseases such as diabetes, leading to misdiagnosis.
Clinical Case:
We present the case of a 70-year-old man with a history of type 2 diabetes mellitus who was admitted to the outpatient clinic due to dysuria and frequent urination. On physical examination, the right testicle was hard, not painful. The ultrasound showed signs of epididymal abscess in the scrotal wall of the right testis, so an infected neoplasm is suspected, performing a right orchiectomy. Later in the histological study, they show giant multinucleated Langhans-type cells with granulomatous areas suggestive of tuberculosis, so it is suggested that in the presence of urological symptoms in patients immunosuppressed tuberculosis is ruled out.
Keywords: Tuberculosis; Orchitis; Epididymitis; Hyperglycemia. (Source : MeSH - NLM).
INTRODUCTION
Around 15% of extrapulmonary TB represents genitourinary tuberculosis; since it is the second common manifestation in the countries of Europe. Commonly infected sites are the epididymis, seminal vesicle, prostate, and testes1.
Genital TB is rare, and testicular TB is even more infrequent, comprising only 3%. Thus, scrotal infection by Mycobacterium tuberculosis occurs in 7% of patients1; being the most common site of genital TB, the epididymis, followed by the seminal vesicles, the prostate, the testicles, and the vas deferens. As the epididymis is affected first, orchitis occurs by contiguous extension and reflects a late stage of the disease. Other authors postulate dissemination through the pelvic lymphatic system and venereal transmission2, with the most affected middle-aged men.
According to the World Health Organization, in 2016, there were an estimated 10.4 million new cases of active tuberculosis (TB) per year, and 1.8 million deaths in 2015 from Mycobacterium tuberculosis3.
The global prevalence of diabetes is 8.3%; In Latin America, the prevalence of diabetes is 5%. In Peru, there is insufficient epidemiological data on DM: however, some studies suggest a prevalence of 5 to 7%4.
The association between TB and DM was described in the middle of the 20th century. Evidence supports the hypothesis that DM increases the susceptibility to developing TB due to immunodeficiency5. However, the emergence of comorbidities such as HIV / AIDS and diabetes mellitus (DM) jeopardize the goal of global TB elimination by 20506.
In Peru, the evidence on the effect of DM and TB is scarce; Only one cohort study in patients at high risk of resistant TB was associated with 11% with DM7.
Through this case, it is proposed that in the presence of urological symptoms in immunosuppressed patients, tuberculosis should be ruled out before any surgical procedure, on the other hand, it is proposed to analyze the relationship that exists between the state of immunosuppression of patients with DM and the extrapulmonary forms of tuberculosis, emphasizing in the testicular presentation.
DESCRIPTION OF THE CLINICAL CASE
This is a case of a 70-year-old man from Huancayo-Junín, with insulin-dependent diabetes mellitus type 2, prostatectomy 10 years ago, and intermittent urinary infection without response to antibiotic treatment. The patient is admitted with dysuria and frequency of 1-month evolution; He denies contact with tuberculosis, fever, sweating, and weight loss.
On examination: pain in the lower abdomen, PRU positive. Right testicle of hard consistency, not painful; a normal left testicle.
Laboratory analysis: leukocytes 7650 cells/mm3, Hb 16.99 gr/dl, platelets 507000 cells/mm3, glucose 195 mg/dl, glycosylated hemoglobin 7.3%. Urine test: glucose ++, leukocytes and red blood cells 1 per field and BAAR in urine x 2 negative. Prostate-Specific Antigen 2.69ng/ml.
Ultrasound: Right testicle of 34x13x25mm, echo hard structure, signs of epididymal abscess and scrotal wall. Left testicle with normal shape, echostructure, and size (36x14x23mm), without signs of varicocele hydrocele. Grade 3 prostatic hyperplasia and kidney stones.
A testicular neoplasm is suspected and added to the ultrasound findings of an epididymal abscess based on age and physical examination. An infected testicular neoplasm is proposed as a diagnosis, indicating right orchiectomy.
Macroscopic study: right testicle plus epididymis 8x4cm, smooth surface; On cut, yellowish brown stroma with a focus of purulent secretion.
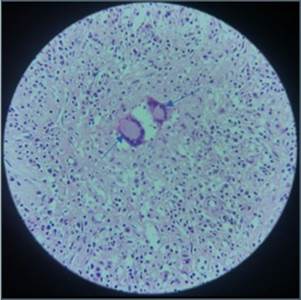
Histopathology: positive acid-fast bacillus (AFB) staining, areas of fibrosis, and mixed inflammatory infiltrate with the presence of giant multinucleated Langhans-type cells with granulomatous areas that defines a diagnosis of tuberculous orchiepididymitis and initiates antituberculous treatment with isoniazid, rifampicin, pyrazinamide, and ethambutol (2HRZE + 4HR) for 6 months. The patient evolved favorably. (Figure 1)
DISCUSSION
Tuberculosis is caused by aerobic, non-motile, airborne Mycobacterium tuberculosis. Pulmonary tuberculosis (TB) is the most common type and represents 70% of cases, spreading especially in immunocompromised patients and young children. The spread of TB to the testicle can result in a secondary infection of the epididymis8.
In relation to the case, we observed an important history of being an insulin-dependent diabetic, therefore an immunocompromised person who, according to the evidence, describes the risk of up to three times more possibilities of becoming infected and developing TB and being able to develop extra-pulmonary disease between 15% and 28%. genitourinary tuberculosis was the outcome of our patient; however, the involvement of other organs such as the prostate, seminal vesicle, vas deferens, testicle, penis, and epididymis is also reported as a frequent complication6. Thus, it is pointed out that genitourinary TB represents 5% of cases of extrapulmonary tuberculosis, the most frequent location being the epididymis, as it was in the case presented7.
At the age of 40 years, urogenital tuberculosis is twice more frequent in men than in women, suggesting that the presence of urinary symptoms and sterile pyuria has renal compromise. On the other hand, a pulmonary alteration can be visualized in the imaging study even in 75%. In our case, the patient reported having presented dysuria and intermittent frequency with an evolution time of up to one month, coinciding with the literature6.; however, no apparent primary pulmonary focus was found since the chest tomography did not show characteristics of having suffered from this disease. (Figure 2)
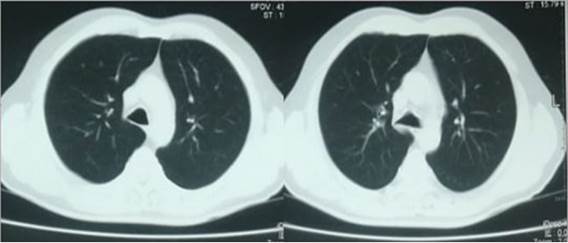
Figure 2: Computed tomography of the chest in the lung window where no tomographic signs of a parenchymal lesion suggestive of tuberculosis are observed
Physical examination findings may include a tender nodule, dilation, and thickening of the epididymis. Testicular involvement can be unilateral or bilateral. Epididymal involvement classically shows up as a heterogeneous hypoechoic mass on ultrasonography. In the urinalysis, albuminuria or hematuria may also be observed. Others report cases of infertility7.
Clinically, it is not usually distinguishable from the testicular tumor, acute infection (bacterial or viral), granulomatous infection (sarcoidosis), or infarction, and can even, in some cases, mimic testicular torsion5. Epididymal enlargement and thickening of the scrotum are the key points of infection.
Testicular ultrasound is currently the best technique for the diagnosis of testicular injury. Here, a great thickening and formation of a dense, caseous mass are observed, which can rupture and give rise to tedious fistulas. Other sonographic findings include thickening of the scrotal skin, hydrocele, calcifications, and scrotal abscess. The addition of Doppler ultrasound serves to assess blood flow and helps differentiate testicular infarction, tumor, or inflammation5.
Regarding the presence of DM, data indicate that having HA1C greater than seven is a risk factor for latent tuberculosis9. In addition, there are differences in the pharmacokinetics of drugs for TB and DM and other comorbidities such as hypertension or obesity, which leads to a higher risk of death and relapse10.
In our case, a patient with immunosuppression, diabetes, compatible symptoms, and histology with epithelioid granulomas, caseous necrosis, and Ziehl-Neelsen staining confirmed the diagnosis.
The evidence recommends antituberculous treatment with the usual regimen of isoniazid, rifampin, pyrazinamide, and ethambutol (2HRZE + 4HR) for 6 months, through which cure rates of 95% are obtained.
However, surgical intervention may be necessary, especially in severe cases, such as no clinical response to treatment, increased testicular size, and edema or abscess formation11.
One of the challenges that occur in patients with DM-TB is therapeutic management since it has been shown that the levels of anti-TB drugs in plasma are below therapeutic values12. This, added to hyperglycemia, makes management difficult.
There are still no randomized studies that evaluate an adequate treatment for TB-DM, and there is not enough evidence to evaluate the effect of insulin or metformin13, with the use of the insulin being recommended in Peru14.
In endemic countries such as Peru, patients with symptoms such as long-standing dysuria and frequency, scrotal mass, or chronic epididymitis should be evaluated for tuberculosis. This would significantly reduce any delay in establishing a diagnosis, increasing the chances of quick management and recovery. A surgical approach should be considered only in cases where the diagnosis is not clearly established or when there is a strong clinical indication. yellowish-brown stroma with a focus of purulent secretion.
REFERENCES
1. WHO. Global tuberculosis report 2016. World Health Organization, Geneva; 2016. http://www.who.int/tb/publications/global_report/en/.Accessed May 12,2017. [ Links ]
2. Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. 2009;9(12):737-46. DOI: 10.1016/S1473-3099(09)70282-8 [ Links ]
3. Miranda JJ, Herrera VM, Chirinos JA, Gómez LF, Perel P, Pichardo R, et al. Major cardiovascular risk factors in Latin America: a comparison with the United States. The Latin American Consortium of Studies in Obesity (LASO). PLoS One.2013;8(1):e54056.DOI: https://doi.org/10.1371/journal.pone.0054056 [ Links ]
4. Magee MJ, Bloss E, Shin SS, Contreras C, Huaman HA, Ticona JC, et al. Clinical characteristics, drug resistance, and treatment outcomes among tuberculosis patients with diabetes in Peru. Int J Infect Dis. 2013;17(6):e404-12. DOI:10.1016/j.ijid.2012.12.029 [ Links ]
5. Muttarak, M and Peh, WC. Case 91: tuberculous epididymo-orchitis. Radiology. 2006; 238: 748-751. DOI: 10.1148/radiol.2382031851 [ Links ]
6. Kapoor R, Ansari MS, Mandhami A, Gulia A. Clinical presentation and diagnostic approach in cases of genitor urinary tuberculosis. Indian J Urol. 2008; 24(3):401-405. DOI: 10.4103/0970-1591.42626 [ Links ]
7. Figueiredo AA, Lucon AM, Srougi M. Tuberculosis urogenital. Microbiol Spectr 2017; 5 (1) 1-16. DOI: 10.1128/microbiolspec.TNMI7-0015-2016 [ Links ]
8. Kumar V, Abbas A, Aster J. Robbins y Cotran. Patología estructural y funcional. Barcelona, España: Elsevier; 2015. p. 371-376. https://www.elsevier.com/books/robbins-y-cotran-patologia-estructural-y-funcional/kumar/978-84-9113-911-9 [ Links ]
9. Martínez G, Serrano C, Castañeda J, Macías N, Hernández N, Enciso L, et al. Associated Risk Factors for Latent Tuberculosis Infection in Subjects with Diabetes. Arch Med Res 2015; 46(3): 221-7. DOI: 10.1016/j.arcmed.2015.03.009 [ Links ]
10. Miranda JJ, Bernabe-Ortiz A, Stanojevic S, Malaga G, Gilman RH, Smeeth L. A1C as a diagnostic criteria for diabetes in low- and middleincome settings: evidence from Peru. PLoS One. 2011;6(3):e18069. DOI: https://doi.org/10.1371/journal.pone.0018069 [ Links ]
11. Baker MA, Harries AD, Jeon CY, Hart JE, Kapur A, Lönnroth K, et al. The impact of diabetes on tuberculosis treatment outcomes: a systematic review. BMC Medicine. 2011;9(1):81. DOI: https://doi.org/10.1186/1741-7015-9-81 [ Links ]
12. Babalik A, Ulus IH, Bakirci N, Kuyucu T, Arpag H, Dagyildizi L, et al. Plasma concentrations of isoniazid and rifampin are decreased in adult pulmonary tuberculosis patients with diabetes mellitus. Antimicrob Agents Chemother. 2013;57(11):5740-2. DOI: 10.1128/AAC.01345-13 [ Links ]
13. Ruslami R, Aarnoutse RE, Alisjahbana B, van der Ven AJ, van Crevel R. Implications of the global increase of diabetes for tuberculosis control and patient care. Trop Med Int Health. 2010;15(11):1289-99. DOI: 10.1111/j.1365-3156.2010.02625.x [ Links ]
14. Perú, Ministerio de Salud (MINSA).Norma Técnica de Salud para la atención integral de las personas afectadas por Tuberculosis. Resolución Ministerial N° 715- 2013/MINSA del 8 de noviembre del 2013. Lima: MINSA; 2013. https://www.gob.pe/institucion/minsa/normas-legales/198713-715-2013-minsa [ Links ]
Received: July 29, 2021; Accepted: October 30, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
