










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.2 Lima abr./jun 2022 Epub 16-Mar-2022
http://dx.doi.org/10.25176/rfmh.v22i2.4393
Clinical case
Goldenhar syndrome associated with an epibulbar dermoid: Case report
1Unidad de Órbita y Oculoplástica, Servicio de Oftalmología, Hospital Nacional Carlos Alberto Seguín Escobedo - EsSalud. Arequipa, Perú
2Universidad Nacional de San Agustín. Facultad de Medicina, Arequipa, Perú
3Universidad Católica Santa María. Facultad de Medicina, Arequipa, Perú
We present the case of a 7-year-old male child with Goldenhar syndrome associated with an epibulbar choristoma. The patient presents a homogeneous tumor, rounded in shape, with well-defined borders, of a soft consistency, vascularized, approximately 9x10 mm, yellowish-white in color, adhered to the sclera and cornea, with hairy formations on its surface, located at the level of the sclerocorneal limbus of the temporal-lower quadrant of his right eye. The histopathology study showed the presence of hair follicles and sebaceous glands, immersed in a stroma of fibrous connective tissue with a superficial squamous-type lining, which defined the diagnosis of limbar epibulbar dermoid. Conjunctivaplasty was performed to cover the scleral defect and use amniotic membrane to cover the corneal and scleral defect. The limbar epibulbar dermoid is the most common type of conjunctival choristoma and should be considered in the differential diagnosis of pediatric epibulbar tumors.
Keywords: Goldenhar syndrome; epibulbar choristoma; epibulbar dermoid. (Source : MeSH - NLM).
INTRODUCTION
Goldenhar syndrome (GS), also known as hemifacial microsomia and oculo-auriculo-vertebral dysplasia, was described by the first time by Von Arlt in 1854 and later named after Dr. Maurice Goldenhar, who reported 3 cases in 1952.1,2
The precise etiology is still unknown, it is a complex developmental disorder during fetal life, which mainly affects structures of the head and neck derived from the first and second brachial arches. It is a rare disease and has a prevalence of 1:3500 to 1:7000 live births, it is more common in men than in women, with a ratio of 3:2 respectively. In 85% of cases, only one side of the face is affected, with right-sided involvement being the most common.1,3
There is no consensus in the literature about the diagnostic criteria for GS. Currently, the diagnosis depends on the clinical manifestations, which include the classic triad: 1) mandibular hypoplasia, resulting in facial asymmetry, 2) ocular and auricular malformations, and 3) vertebral anomalies. Other skeletal, ocular, renal, and cardiac anomalies have been described.1,4
In relation to ocular manifestations, they are most commonly represented by colobomas of the upper eyelid associated with iris/chorioretinal coloboma, epibulbar choristoma (epibulbar dermoid and conjunctival lipodermoid) and, less frequently, microphthalmia/anophthalmia, strabismus, cataracts or cleft asymmetry eyelids.5,6
Epibulbar dermoid represents one of the most common forms of the various ocular manifestations that occur in GS; It can be eccentric or limbal and has the following characteristics: it is a soft, localized, elevated, opaque, yellowish-white mass at the limbus, with full-thickness corneal involvement, sometimes with hair follicles on the surface. The most common location is temporal-inferior, but choristomas of the nasal limbus have been reported. It is necessary to determine the extent of the lesion, if there is suspicion of intraocular involvement, it is decided to perform an ultrasonic biomicroscopy (UBM); if orbital extension is suspected, computed tomography (CT) or magnetic resonance imaging (MRI) may be performed.5,7
The treatment of the epibulbar dermoid can be conservative (periodic observation) or surgical, depending on the size and the involvement of the cornea and anterior chamber. Regarding surgical treatment, a combination of excision, lamellar keratoplasty and amniotic membrane resurfacing, and limbal stem cell transplantation is recommended. The goal of treatment is to prevent amblyopia (caused by irregular astigmatism or visual axis obstruction) or by cosmetic considerations.7,8
We present the case of a patient with a Goldenhar Syndrome diagnosis, carrier of an epibulbar limbal dermoid in the right eye (RE), we discuss the surgical management and postoperative evolution. The relatives authorized the publication of the clinical case and explicit photographs through informed consent.
CASE PRESENTATION
A 7-year-old male schoolboy from Arequipa, diagnosed with Goldenhar Syndrome, who underwent surgery on several occasions for multiple congenital malformations (cleft lip, preauricular appendages, and mandibular hypoplasia), whose mother reported a tumor in the RE present since birth. birth, which has been increasing in size over the last few years, and which causes tearing and difficulty closing the eyelid of the RE. (Figure 1).

Figure 1: Craniofacial malformations. Mandibular hypoplasia that causes facial asymmetry, eye and hearing malformations, which are characteristic of Goldenhar Syndrome. (Source: Clinical History)
On ophthalmological examination, he presented a best corrected visual acuity (BCVA) of 20/70 in the right eye (RE) and 20/20 in the left eye (LE). An intraocular pressure of 13 mmHg in the RE and 12 mmHg in the LE is found. Examination of the anterior segment of the RE revealed a homogeneous tumor, round in shape, with well-defined borders, soft, vascularized, approximately 9x10 mm, yellowish-white in color, adhered to the sclera and cornea, with hairy formations in the its surface, located at the level of the sclerocorneal limbus of the temporal-inferior quadrant; no alterations were found in the LE during the evaluation (Figure 2). There were no abnormalities in the intrinsic or extrinsic ocular motility tests and normal Cover Test. The fundus examination was normal in both the RE and the LE.

Figure 2: RE epibulbar dermoid. Epibulbar tumor at the level of the temporal-inferior quadrant, round in shape, approximately 9X10 mm, yellowish-white in color. (Source: Clinical History)
An image study with CT of the RE orbit is requested, which rules out orbital involvement. The UBM of RE shows that at the level of the temporal-inferior quadrant, on the corneal surface there is a homogeneous lesion, with defined borders, of approximately 2.59 mm in maximum height and 9.85 mm in extension, with a cleavage plane between the corneal tissue and the lesion whithout signs of infiltration of the cornea or the anterior chamber. Thinning of the corneal tissue under said lesion is also observed, ranging from 0.39 mm to 0.42 mm (Figure 3).
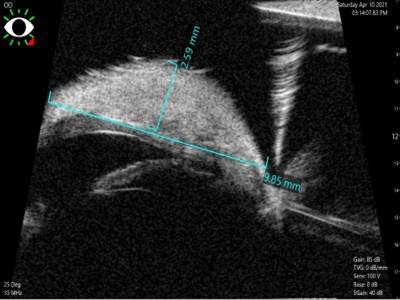
Figure 3: UBM of RE epibulbar dermoid. Homogeneous lesion located on the corneal surface in the inferior temporal quadrant, with a maximum height of approximately 2.59 mm and an extension of 9.85 mm, without infiltration of the cornea or the anterior chamber. (Source: Clinical History)
Due to the characteristics described, a benign corneal-conjunctival tumor is proposed as a possible diagnosis: limbal epibulbar dermoid. A sclerotomy and lamellar keratectomy with a No. 15 scalpel blade are performed to remove the epibulbar tumor for cosmetic purposes and to reduce the risk of amblyopia. The ocular surface defect is reconstructed, conjunctivoplasty is performed to cover the scleral defect and amniotic membrane is used to cover the corneal and scleral defect, the latter is fixed to the perilimbar conjunctiva with 10/0 nylon.
The sample is sent to the Pathological Anatomy Service, the microscopic analysis reports subepithelial fibrous tissue, with hair follicles, sebaceous glands surrounded by conjunctival epithelium and moderate perifollicular lymphocytic infiltrate compatible with the diagnosis of an epibulbar limbal dermoid-type conjunctival choristoma (Figure 4).
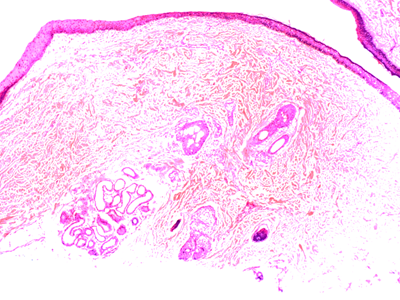
Figure 4: Histopathology of the epibulbar limbal dermoid of RE: Microscopic examination reveals subepithelial fibrous tissue, with hair follicles, sebaceous glands surrounded by conjunctival epithelium, and moderate perifollicular lymphocytic infiltrate. (Source: Clinical History)
Postoperative treatment with Ciprofloxacin and topical Dexamethasone for three weeks is indicated. Postoperative evolution was satisfactory. The stitches were removed at three weeks, by which time the ocular surface had regenerated and the amniotic membrane had disintegrated. There were no postoperative complications. Three months later, the clinical evolution is favorable: he is asymptomatic, on physical examination the BCVA of the RE is 20/30, the formation of an avascular corneal leukoma in the temporal-inferior quadrant is evident, corresponding to the area affected by the tumor, conjunctiva normal in appearance, no signs of recurrence of the lesion can be seen (Figure 5).

DISCUSSION
Epibulbar choristoma represents normal tissue proliferating in an abnormal location; It is a rare entity, with a reported incidence between 1/10,000 and 1/30,000. Histopathologically, they are classified into 4 groups: dermoids, dermolipomas, complex choristomas, and single-tissue choristomas. Limbal epibulbar dermoid is the most common type of epibulbar choristoma; it is characterized by being well circumscribed, being a dome-shaped keratinized limbal mass and being located inferotemporally9,10, as in the present case.
Epibulbar choristomas are normally characterized by being sporadic and can develop alone, however, they can occasionally appear associated with different systemic syndromes, such as Goldenhar syndrome, epidermal nevus syndrome, Haberland syndrome, oculo-cerebro-cutaneous syndrome and oculodermal syndrome.11, in the present case it was associated with Goldenhar Syndrome.
These lesions can cause amblyopia and strabismus, although with early identification and excision of limbal epibulbar dermoid lesions, amblyopia and strabismus can be avoided, and thus improve the visual prognosis of patients with Goldenhar syndrome12, as happened in the present case.
The anatomopathological study showed the presence of hair follicles and sebaceous glands, immersed in a stroma of fibrous connective tissue with a superficial scaly-type coating, as mentioned in the literature.13,14
Infiltration of the cornea and sclera by these tumors is rare, and in these cases excision of the lesion and reconstruction by means of a conjunctivoplasty is not usually sufficient; in these cases amniotic membrane coverage is indicated.12,15
The amniotic membrane is used to act as a substrate for the migration of epithelial cells, which can easily replicate, and achieve regeneration of the conjunctival-corneal epithelium and also reconstruction after the removal of both malignant and benign tumors15,16, due to all these characteristics we resorted to amniotic membrane coverage in the present case.
CONCLUSION
Goldenhar syndrome is rare and has a very varied spectrum presentation among patients. This pathology is characterized by an abnormal development of several craniofacial structures, such as the eyes, which have epibulbar choristomas as their classic presentation.
As it is a congenital pathology, manifestations should be taken into consideration early and assess how to worsen normal visual development.
Limbal epibulbar dermoid is the most common type of epibulbar choristoma and should be considered in the differential diagnosis of epibulbar tumors located in the temporal-inferior quadrant.
Histopathological study is important to confirm the diagnosis and rule out malignant lesions. Excision of the tumor is indicated in the presence of symptoms or in case of progressive growth; In cases of extensive tumors, the use of amniotic membrane coating is indicated, due to its regeneration properties of the conjunctive-corneal epithelium and being a substrate for the migration of epithelial cells.
REFERENCES
1. Ding X, Wang X, Cao Y, et al. Goldenhar syndrome with blepharophimosis and limb deformities: a case report. BMC Ophthalmo1.2018;206(18):1 -5. https://doLorg/10.1186/s12886-018-0872-5 [ Links ]
2. Brue C, Mariotti C, Celani 5, et al. A case of Goldenhar syndrome associated with a new retinal presentation: exudative vitelliform maculopathy. Case RepOphthalmolMed.2015;1:1-4. https://doi.org/10.1155/2015/626027 [ Links ]
3. Torres C. Goldenhar syndrome: Clinical manifestations and literature review. Pediatr Panama. 2020;49(1):17-20. DOI: 10.37980/im.journal.rspp.20201591 [ Links ]
4. Martelli H, Teixeira R, Fernandes C, et al. Goldenhar syndrome: clinical features with orofacial emphasis.J Appl Oral Sci.2010;18(6):646-649. DOI: 10.1590/S1678-77572010000600019 [ Links ]
5. Schmitzer 5, Burcel M, Dascalescu D, Popteanu I. Goldenhar Syndrome - ophthalmologist's perspective. Rom J Ophthalmol.2018;62(2):96-104. DOI: 10.22336/RJO.2018.15 [ Links ]
6. Ashokan C, Sreenivasan A, Saraswathy G. Goldenhar syndrome - review with case series.J Clin Diagn Res. 2014;8(4)1 7-19. DOI: 10.7860/JCDR/2014/7926.4260 [ Links ]
7. Pirouzian A. Management of pediatric corneal limbal dermoids. Clin Ophthalmo1.2013; 7:607-614. http://doLorg/10.2147/OPTH.S38663 [ Links ]
8. Tapia A, Merino P, Perez P, et al. Epibulbar Choristoma in Goldenhar syndrome: when to treat to prevent amblyopia?. Acta Estrab. 2015;44(2)1 85-188. https://www.estrabologia.org/actas/Acta_2_2015/12_com_corta.pdf [ Links ]
9. Hsia Y, Lien H, Wang I, Liao 5, et al. Epibulbar complex choristoma with simultaneous involvement of eyelid: a case report. BMC Ophthalmol. 2019;19:1-4. https://doLorg/10.1186/s12886-019-1234-7 [ Links ]
10. Arenas F, Muro P, Urbano E, et al. Coristoma Oseo epibulbar: caso clinic° y revision de literatura. Arch Soc Esp Ofta Imo!. 2020; 95(6):289-292. https://doi.org/10.1016/j.ofta1.2020.02.005 [ Links ]
11. Aldossary M, Alkatan H, Maktabi A. Epibulbar complex and osseous choristoma: Clinicopathological study with interesting associations. Ann Med Sur.2018;36:135-141. https://doi.org/10.1016/j.amsu.2018.10.027 [ Links ]
12. Brue C, Mariotti C, Celani S, et al. A case of Goldenhar Syndrome Associated with a New Retinal Presentation: Exudative Vitelliform Maculopathy. Case Rep Ophthalmol. 2015; 1:1-4. http://dx.doi.org/10.1155/2015/626027 [ Links ]
13. Alarcon T, Bernal G, Salcedo G, et al. Coristomas epibu !bares. Caracteristicas clinicopatolOgicas. Rev Mex Oftalmol. 2004; 78(4): 182- 187. https://www.medigraphic.com/pdfs/revmexoft/rmo-2004/rmo044e.pdf [ Links ]
14. Pal 5, Bose K, Chakrabarti S, Mondal A. Limbal complex choristoma - A rare unexpected lesion diagnosed by histopathology. Clin Cancer Investig J. 2017; 6(5):227-229. DOI: 10.4103/ccij.ccij_53_17 [ Links ]
15. Walkden A. Amniotic Membrane Transplantation in Ophthalmology: An Updated Perspective. Clin Ophthalmo1.2020; 14: 2057-2072. https://doi.org/10.2147/OPTH.S208008 [ Links ]
16. Lacorzana J. Amniotic membrane, clinical applications and tissue engineering. Review of its ophthalmic use. Arch Soc Esp Oftalmol.2019; 95 (1):15-23. https://doi.org/10.1016/j.ofta1.2019.09.010 [ Links ]
Received: June 12, 2021; Accepted: December 17, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
