










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.4 Lima oct./dic. 2022 Epub 12-Oct-2022
http://dx.doi.org/10.25176/rfmh.v22i4.5046
Clinical case
Decreasing hypoglycemia unawareness in a patient with type 1 diabetes mellitus after continuous glucose monitoring: tools for self-care
1Hospital María Auxiliadora, Lima, Perú.
3Universidad de Florida. Gainesville, Florida, USA.
4Universidad Peruana Cayetano Heredia. Lima, Perú.
5Universidad Científica del Sur. Lima, Perú.
Diabetes mellitus is a public health problem that causes early and late complications. Continuous glucose monitoring (CGM) has become the main technological tool for real-time glycemic control and has the potential to prevent complications. However, its use has not spread in low- and middle-income countries. We present the experience in the management of a patient with type 1 diabetes with hypoglycemia unawareness in whom the use of real-time CGM achieved both: less hypoglycemic episodes and optimization of insulin regimen. The benefit of real-time CGM in addition to the use of analog insulins and diabetes education resulted in better metabolic control. CGM is a useful tool to consider in patients with hypoglycemia unawareness and to minimize the risk of complications in the future.
Keywords: Diabetes mellitus type 1; Technology; Education; Blood Glucose Self-Monitoring; Hypoglycemia. (Source: MeSH NLM).
INTRODUCTION
Type 1 diabetes mellitus (DM1) represents between 5 to 10% of all diabetes cases and is a condition where beta cells are destroyed by an autoimmune phenomenon. The prevalence and incidence of DM1 are approximately 5.6 and 15 cases per 100,000 inhabitants, respectively, worldwide1, with the number of new cases in children and young people during the COVID-19 pandemic being alarming2.
In Peru, the incidence is low, with approximately one case per 100,000 inhabitants in children under 15 years of age3, but it is increasing. Recently, the National Institute of Child Health in Peru reported a greater number of new cases per year between 2011 and 20184. Patients with DM1 have greater difficulty in reaching glycated hemoglobin (HbA1c) goals and thus be able to reduce complications. Fear of hypoglycemia and poor adherence to treatment in these patients greatly affect good glycemic control. In parallel, hypoglycemia increases mortality and cardiovascular risk5.
Self-monitoring is essential for the control of DM1; however, the cost of fingerstick glucose monitoring and the discomfort and pain associated with it limits its use. In developed countries, the use of continuous glucose monitoring (CGM) has become the main technological tool for real-time glycemic control. In Peru, there is a previous report on the use of CGM in an adult6and a retrospective study of 28 patients between children and adults7.
In this report, we describe the case of a patient with DM1 with poor metabolic control and recurrent hypoglycemia in whom the use of real-time CGM reduced hypoglycemic episodes, improved quality of life, and reached the appropriate dose of insulin.
DESCRIPTION OF THE CLINICAL CASE
A 39-year-old female patient from the northern region of Peru, with a personal history of two previous abortions and DM1 since she was 23 years of age, with a report of an episode of diabetic ketoacidosis currently undergoing treatment with insulin therapy. On the first visit, the patient is evaluated by teleconsultation due to confinement due to the COVID-19 pandemic. Capillary glucose was measured 1 or 2 times a day, 50-70% of the time with a value less than 70 mg/dl, several of the episodes were asymptomatic. She suffered from almost daily episodes of hypoglycemia either day and/or night, with documented symptoms up to approximately 35mg/dl of capillary glucose, some of them were severe nocturnal hypoglycemia that required the assistance of another family member with glucose reaching up to 23 mg/dl.
He has a history of an arm fracture due to severe hypoglycemia with loss of consciousness. His height is 163 cm and weight 49 Kg (BMI 18.4 Kg/m2), body mass index is usually less than 20 Kg/m2, he used NPH and Regular insulin with a total daily dose of insulin (TDD) 1 at 1.2 IU/KG (seeTable 2). Auxiliary tests showed the following results: HbA1c 8.1%, C-peptide <0.01 nmol/L, total cholesterol: 197 mg/dl, high-density lipoprotein (HDL) 56 mg/dl, low-density lipoprotein (LDL) 138 mg/dl, triglycerides: 65mg/dl, thyroid-stimulating hormone (TSH): 1.52mIU/L, creatinine 1.44mg/dl, and microalbuminuria 1.4mg/L.
Six days after the teleconsultation, a Free Style Libre 2 CGM sensor was placed. Given the high dose of daily insulin and the high frequency of hypoglycemia, the change to insulin analogs was made according to weight: glargine 18 IU/day and lispro 4/7/5 IU before breakfast, lunch, and dinner, respectively, while providing nutritional education and counseling (seeTable 2). Following the manufacturer's instructions, the sensor was applied to the skin of the outer aspect of the arm. Likewise, the Libre 2 scanner was provided and he was instructed to scan the CGM sensor at least every 8 hours during the 14 days that the sensor lasts. The patient sent daily insulin dose information and photos of her food. Correction of insulin doses was coordinated with her and the accuracy of carbohydrate counting was reinforced. Additionally, during the 2 weeks of CGM use, the patient made her own minimal adjustments to the basal and preprandial insulin doses, empowering her in the education and management of her diabetes.
Table 1. Anthropometric and biochemical data during follow-up.
| At the beginning | at 4 months | |
|---|---|---|
| BMI (weight/m2) | 18,44 | 18,06 |
| Weight (kg) | 49,0 | 48,0 |
| HbA1C (%) | 8,1 | 7,3 |
| Hemoglobin (g/dl) | - | 13,4 |
| Uric acid (mg/dl) | - | 3,2 |
| Total cholesterol (mg/dL) | 197 | 162 |
| Cholesterol HDL (mg/dL) | 56 | 46,6 |
| Cholesterol LDL (mg/dL) | 138 | 104,9 |
| Triglycerides(mg/dL) | 65 | 63,8 |
| Creatinine(mg/dL) | 1,44 | 0,94 |
| TGP or Alanine Aminotransferase (mUI/mL) | - | 19 |
| 24-hour microalbuminuria(mg/L) | 1,4 | - |
| C-peptide (nmol/L) | <0,01 | - |
| TSH (mUI/L) | 1,52 | - |
The report of the first CGM obtained a time in the range of 70 to 180 mg/dl in 66% (the hypoglycemia alarm setting was from 70 mg/dl), an average glucose of 134 mg/dl, a glucose variability 46.2% and 26 low glucose events with an average duration of 120 minutes (Figure 1). The basal insulin dose was 18 IU/day and preprandial insulin was finally divided into 2/2/2 IU on average (Table 2).
Table 2. Daily Insulin Dose and Continuous Glucose Monitor Data.
| Before the use of the CGM | First CGM | Second CGM | ||
|---|---|---|---|---|
| Daily dose of insulin (IU) | 1,04 - 1.2 UI/Kg/day | 0,57 UI/Kg/day | 0,62 UI/Kg/day | |
| Basal insulin(UI) | NPH 25 and 20 UI | Glargine U-100 18 UI | Glargine U-100 21 UI | |
| Preprandial insulin (UI) | Regular -/10/- UI | Lispro 2/2-3/2 UI | Lispro ~3/3/3 UI | |
| Average glucose (mg/dl) | 134 | 137 | ||
| Glucose variability (%Standard deviation/mean) | 46,2% | 45,6% | ||
| Glucose Management Indicator (GMI) or estimated HbA1c | 6,5% | 6,6% | ||
| Time in Range 70-180 mg/dl | 66% | 70% | ||
| Time between 54 and 69 mg/dl | 12% | 8% | ||
| Time below 54 mg/dl | 2% | 2% | ||
| Time above 180mg/dl | 14% | 13% | ||
| Time above 250mg/dl | 6% | 7% | ||
| Low glucose events | 26 | 18 | ||
| Mean duration of hypoglycemic episode (minutes) | 120 | 117 | ||
| Total duration of hypoglycemia in 14 days | 3120 minutes 52 hours or 3.8 hours/day | 2106 minutes 35.1 hours or 2.5 hours/day | ||
| Treatment changes | Before sensor | daily dose of insulin (UI) | 0,69 UI/Kg/day | 0,58 UI/Kg/day |
| Basal Insulin UI) | Glargine U-100 18 UI | Glargine U-100 18 UI | ||
| Preprandial insulin (UI) | Lispro 5/7/4 UI | Lispro 2-4/2-4/2 UI | ||
| After sensor | Daily Insulin Dose(UI) | 0,57 UI/Kg/day | 0,62 UI/Kg/day | |
| Basal Insulin (UI) | Glargine U-100 18 UI | Glargine U-100 21 UI | ||
| Preprandial insulin(UI) | Lispro 4/2-4/2 UI | Lispro ~3/3/3 UI | ||
At the four-month outpatient follow-up, she showed better control of self-monitoring of glucose, with capillary glucose measurement four times a day, and fewer hypoglycemia episodes. It was decided to install another CGM for two weeks, with an alarm setting from 80mg/dl to prevent hypoglycemic episodes earlier. An average glucose value of 137 mg/dl, a target range at 70%, a glucose variability of 46.6% and 18 low glucose events with an average duration of 117 minutes were recorded (SeeFigure 1). Control laboratory tests showed the following results: HbA1C: 7.3%, total cholesterol 162 mg/dl, HDL 46.4 mg/dl, LDL 104.9 mg/dl, triglycerides 63.8 mg/dl, creatinine 0.4 mg/dl, TGP or Alanine Aminotransferase 19 mIU/mL.
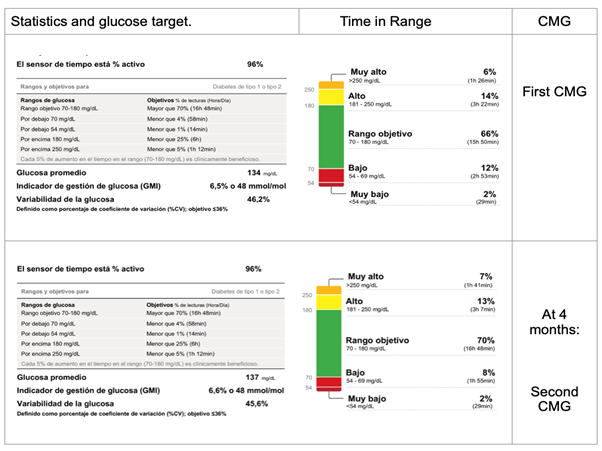
Figure 1 Report of glucose statistics and time in range using Continuous Glucose Monitor MCG: FreeStyle Free 2 Continuous Glucose Monitor
The dose at four months of basal insulin with insulin glargine was 21 IU/day and insulin lispro 3/3/3 IU/day. The patient reports less hypoglycemia and better quality of life, in addition to a better understanding of the effect of the number of carbohydrates, which allows her to have more control over the disease.
DISCUSSION
Hypoglycemia causes cognitive impairment and is associated with mortality in 4-10% of patients with DM1, and cases have been described of patients dying during sleep after long periods of asymptomatic hypoglycemia9,10. In the present report, our patient decreased the number of hypoglycemic events between the first and second CGM from 24 to 18 episodes, respectively. Although the average duration was similar (120 minutes versus 117 minutes), the total time of hypoglycemia in the 14 days that each GCM lasted decreased from 3120 minutes (3.8 hours per day) in the first GCM to 2106 minutes (2.5 hours per day) in the second GCM. The higher the frequency of hypoglycemia, the higher the reactive hyperglycemia due to the fear of a hypoglycemic episode9. Recently, international guidelines, in addition to glycosylated hemoglobin, recommend goals based on the GCS as the longest time in range, the shortest time in hypoglycemia and the lowest glycemic variability to mitigate long-term complications11.
In the case of our patient, she reported a decrease in hypoglycemia episodes with the switch to insulin analogs. This suggests that, with the previous regimen of NPH and regular with which she had higher daily insulin doses, the exposure to daily hypoglycemia was probably even worse. The use of real-time CGM allowed the patient to better understand the impact of carbohydrate intake and its relationship to insulin doses.
The availability of hypoglycemia alarms on the MCG is especially useful in patients with a history of asymptomatic hypoglycemia as in our patient. Many of the episodes of hypoglycemia are nocturnal and the alarm shortens the time of exposure to hypoglycemia, as was observed in a pediatric patient who did not react to hypoglycemia when using a CGM without a hypoglycemia alert, but did when she switched to a CGM with alerts that helped reduce the duration of hypoglycemia12.
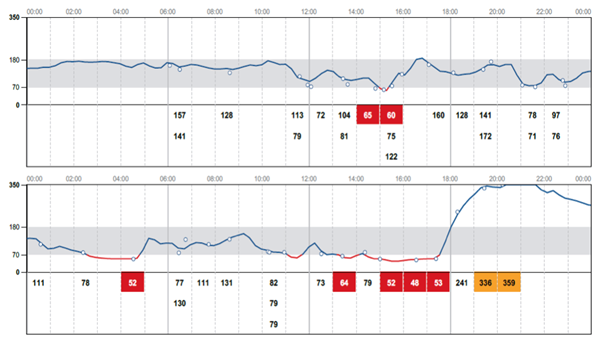
Of special interest is the patient's lack of reaction to the MCG hypoglycemia alert as seen inFigure 2. The upper panel shows 20 scans (white circles), two of them with hypoglycemia around 3 PM. The previous 15 hours there was no hypoglycemia. The glucose level is seen to rise 20 minutes after hypoglycemia was detected. The next day the patient had a 2-hour episode of hypoglycemia between 2:20 and 4:40 AM. She scanned the MCG at 4:30 which yielded a value of 52 and within minutes her glucose level began to rise indicating carbohydrate intake. However, in the afternoon of the same day she had a prolonged episode of hypoglycemia between 1pm and 5:30pm. The patient performed several scans approximately 1 per hour, several of them corresponding to hypoglycemia, but the glucose level remained at about the same level suggesting no carbohydrate intake until 5:30pm, when she developed marked reactive hyperglycemia, greater than 300 mg/dL for several hours, suggesting excessive carbohydrate intake.
Hypoglycemia is known to transiently and sometimes permanently affect cognitive function13, it is possible that the frequent episodes of hypoglycemia, especially that of the same day, may have affected the patient's decision-making ability, predisposing her to develop more hypoglycemia that same day in the afternoon.
In a previous report, the case of a 29-year-old patient with long-standing DM1 who used a blinded CGM (Lizarzaburu) was described. The blinded CGM does not show the patient the glucose level in real time but at the end of the period of use (6 to 14 days later), in the mentioned case, the CGM showed a time in target range of 17% and persistent hyperglycemia, it is mentioned that there was lack of adherence to nutritional control and physical activity; subsequent controls at the third and fifth year showed gradually less hyperglycemia, better glycemic control (HbA1c) and with little evidence of hypoglycemia, however, she reached a higher BMI than at the beginning.
To our knowledge, the present report is the first Peruvian case of improvement of severe hypoglycemia and decrease in the frequency of asymptomatic hypoglycemia with the use of CGM in DM1. In addition to visualizing her glucose level, the patient had a very close medical and nutritional follow-up, which enhanced nutritional education and empowerment. This improvement continued after 4 months of follow-up when she even increased the time in target range from 66% during the first CGM to 70% in the second CGM, in addition to a clinically significant reduction of 1.3 hours of hypoglycemia per day.
In our setting, a pilot study of 28 patients in pediatric and adult populations showed that the use of the CGM, although for a short period of time, was beneficial in either type 1 diabetes (predominantly children) or type 2 diabetes (predominantly adults). In that study, those who used the Free 14-day MCG system with scanning, but without a hypoglycemia alarm, there was a correlation between the number of scans and time in the range 70-180 mg/dl, while adults who used the blinded monitor had no behavioral feedback of carbohydrate intake as the patient was "blind" to the glucose level7. 100 years after the discovery of insulin, patients with diabetes have empowered their diabetes treatment thanks to more stable and predictable insulins in their absorption (analogs) and the GCM technology that allows an approach to the ideal therapy of the patient with DM1. In conclusion, the CGM, especially incorporating an alarm system, is a useful tool to consider in patients with diabetes and asymptomatic hypoglycemia as it allows an optimization of the insulinization schedule therapy, empowerment of the patient with carbohydrate intake and insulin use, and a clinically significant decrease in the frequency and total duration of hypoglycemia.
REFERENCES
1. American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Supplement 1):S15-33; doi: 10.2337/dc21-S002. [ Links ]
2. Kamrath C, Mönkemöller K, Biester T, Rohrer TR, Warncke K, Hammersen J, et al. Ketoacidosis in Children and Adolescents With Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic in Germany. JAMA. 2020;324(8):801-4; doi:10.1001/jama.2020.13445 [ Links ]
3. Seclén S, Rojas MI, Nuñez O, Valdivia H, Millones B. Registro de 10 años de incidencia (1985-1994) de Diabetes Mellitus Tipo 1 en población infantil peruana. Diagnóstico. 2002; 41(2):54-62. [ Links ]
4. Díaz-Martinez LE, Del Aguila CM, Falen JM, Rojas MI, Nuñez O, Chavez EM, et al. Características Clínicas, Bioquímicas y Ambientales al Debut De Pacientes Con Diabetes Mellitus Tipo 1 En El Instituto Nacional De Salud Del Niño, Perú. Rev Perú pediatr. 2021 [citado 7 de noviembre de 2021]; 74(02):09-11. Disponible en: https://pediatria.org.pe/wp-content/uploads/2021/10/VOL-74-Nro-02-2021.pdf [ Links ]
5. Davis AK, DuBose SN, Haller MJ, Miller KM, DiMeglio LA, Bethin KE, et al. Prevalence of detectable C-Peptide according to age at diagnosis and duration of type 1 diabetes. Diabetes Care. 2015;38(3):476-81. doi:10.2337/dc14-1952. [ Links ]
6. Lizarzaburu JC, Vera JM, Chia SG. Paciente adulto con diabetes mellitus tipo 1: múltiples factores para lograr un control adecuado. Reporte de caso. Horiz. Med. [Internet]. 2020 Oct; 20 (4): e1166. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1727-558X2020000400014&lng=es. http://dx.doi.org/10.24265/horizmed.2020.v20n4.14. [ Links ]
7. Zhang C, Angulo J, Sotil K, Acho E, Manrique H, Vélez M, Leey J. Características glucométricas del monitoreo continuo de glucosa en el manejo de diabetes mellitus en niños y adultos de Lima, Perú. Un estudio preliminar. Revista De La Sociedad Peruana De Medicina Interna. 2022, 35(2), 54-58. [ Links ]
8. FreeStyle Libre 2. Indications and Important Safety Information [Internet]. FreeStyle Abbott. 2022 [cited 2022 June 24]. Available from: https://www.freestyle.abbott/us-en/safety-information.html [ Links ]
9. DiMeglio LA, Evans-Molina C, Oram RA. Type 1 diabetes. Lancet Lond Engl. 2018;391(10138):2449. doi:10.1016/S0140-6736(18)31320-5. [ Links ]
10. Tanenberg RJ, Newton CA, Drake AJ. Confirmation of hypoglycemia in the "dead-in-bed" syndrome, as captured by a retrospective continuous glucose monitoring system. Endocr Pract. 2010 Mar-Apr;16(2):244-8. doi: 10.4158/EP09260.CR. PMID: 19833577. [ Links ]
11. Holt RIG, DeVries JH, Hess-Fischl A, Hirsch IB, Kirkman MS, Klupa T, et al. The Management of Type 1 Diabetes in Adults. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2021;44(11):2589-625. doi: 10.2337/dci21-0043. [ Links ]
12. Angulo J, Zhang C, Manrique H, Leey J. Hypoglycemia Detection Using an Electronic Alarm System with Continuous Glucose Monitoring: A Case Report. Rev Peru Pediatr 2021, 74 (2): 31-36. [ Links ]
13. Fanelli CG, Paramore DS, Hershey T, Terkamp C, Ovalle F, Craft S, Cryer PE. Impact of nocturnal hypoglycemia on hypoglycemic cognitive dysfunction in type 1 diabetes. Diabetes. 1998 Dec;47(12):1920-7. doi: 10.2337/diabetes.47.12.1920. PMID: 9836525. [ Links ]
14. Bäßler, J. & Schwarzer, R. (1996). Evaluación de la autoeficacia: Adaptación española de la escala de autoecacia general [Measuring generalized self-beliefs: A Spanish adaptation of the General Self-Efficacy scale]. Ansiedad y Estrés, 2(1), 1-8. [ Links ]
8Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0(https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: July 18, 2022; Accepted: October 14, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
