










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.23 no.1 Lima Jan./Mar. 2023 Epub Jan 25, 2023
http://dx.doi.org/10.25176/rfmh.v23i1.5059
Original Article
Factors associated with hemoglobin levels in children under 6 months of age hospitalized in a pediatric center in Peru
1Universidad Científica del Sur. Lima, Peru.
2Instituto Nacional de Salud del Niño. Lima, Peru.
3Escuela de Posgrado, Universidad Continental. Lima, Peru.
4Universidad Peruana de ciencias aplicadas. Lima, Peru.
Introduction:
Anemia is a condition in which there is a low concentration of hemoglobin (Hb) levels. Although many causes of anemia have been identified, there are few studies in which they are related to epidemiological factors in the first months of life.
Objective: to determine the factors associated with hemoglobin levels in children under 6 months of age hospitalized in a specialized pediatric center in Peru.
Methods:
Cross-sectional study of children under 6 months of age hospitalized in the medical services of a pediatric center in 2017; 267 medical records were reviewed, emphasizing clinical and epidemiological characteristics.
Results:
61.4% of the infants were women, and only 6.7% of the population studied were less than 1 month old. 6.7% had a low birth weight, and 53.2% had a normal delivery. The level of anemia in hospitalized children under 6 months of age is 66.7%.
Conclusions:
According to the bivariate analysis, a significant association is found between hemoglobin levels with the variables age, nutritional status, weight for length, and hospital causes. Regarding the multivariate analysis, only an association was found between age and the median Hb in boys and girls aged 0 to 5 months hospitalized in a pediatric center in Peru.
Keywords: child, hospitalized; anemia, iron-deficiency; epidemiologic study characteristics; hospitals, pediatric.(source: mesh nlm)
Introduction
Anemia is a condition in which there is a low concentration of hemoglobin (Hb) levels and red cell mass compared to the average1. Although many causes of anemia have been identified, there are few studies in which they are related to epidemiological factors in the first months of life.
Worldwide, certain epidemiological factors related to anemia in infants are recognized. Studies carried out in latin american countries have found two epidemiological characteristics associated with the presence of childhood anemia: poverty and low educational levels on the part of the parents.2,3. In addition, these same components have been repeatedly found in countries such as bangladesh and india.4-8.
At the level of Peru, the educational and socioeconomic level of the parents is associated with predisposing factors to anemia.9,10. It is worth mentioning that childhood anemia is a topic of main national interest because 40.1% of boys and girls under three years of age present it.11.
The national institute of child health (INSN) of Peru treats pediatric patients in the hospitalization area for various diseases, including infectious diseases; which, being linked to other epidemiological factors such as nutritional status and anemia, can impact immunity, increasing infant morbidity and mortality12,13. In addition, there are chronic diseases associated with anemia, such as heart failure, cancer, and inflammatory bowel disease.13. For this reason, recognizing factors that predispose to presenting anemia in the first months of life is a strategy to consider to mitigate its prevalence at the national level and, above all, to avoid any in-hospital complication.
The objective of this study was to determine the factors associated with hemoglobin levels in children under 6 months of age admitted to a specialized pediatric center in Peru.
Methods
Cross-sectional analytical study carried out in a specialized hospital in the capital of Peru.
Population and sample
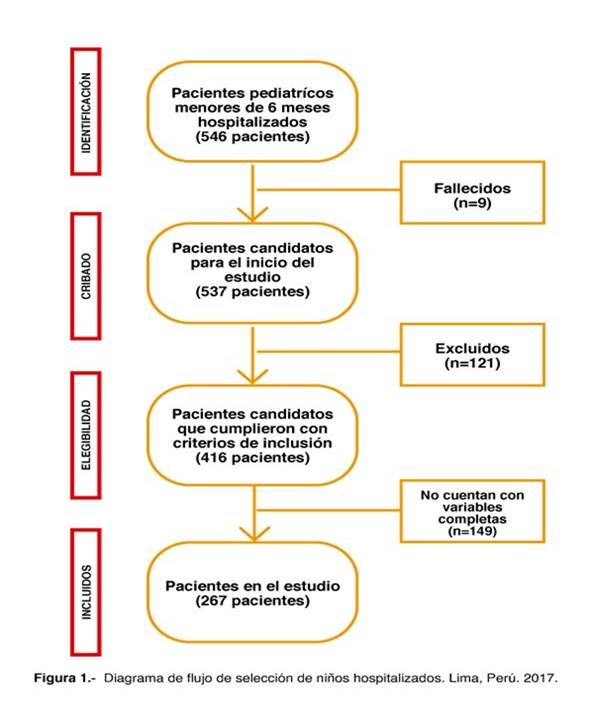
The population consisted of infants under 6 months of age hospitalized in the medical services of the INSN of Peru. A census of hospitalized patients was carried out taking as a reference the hospital discharges of the year 2017, finally 267 hospitalized infants were obtained who met the inclusion criteria of the study, being hospitalized in the INSN medicine services and with complete records of the study variables. In the medical records (figure 1). Those with congenital malformation, genetic disorder, hiv infectio
Variables and instruments
The dependent variable was the hemoglobin (Hb) level, taken on admission to hospitalization, determined from the medical records. For the determination of anemia, the ministerial resolution of the ministry of health of Peru no. 250-2017 was used, which uses the cut-off points pre-established by the who. Anemia was considered in children under 2 months of age with <13.5 g/dl of Hb in blood, and from 2 to 6 months with <9.5 g/dl of Hb in blood(14). The independent variables were birth weight, length at birth, head circumference at birth, delivery characteristics, sex, origin, poverty quintile, age, nutritional status, causes of hospitalization, and hospital stay. The technique was data collection from medical records.
Procedure
Data collection from medical records was performed, with emphasis on clinical and epidemiological characteristics. There was a format designed for the study, the data entered in the formats was entered in an excel spreadsheet for subsequent analysis. To establish the poverty quintiles, the infant's district of residence and the monetary poverty map of Peru were used. The quintiles are a subdivision of the population into 5 partially equal parts, with the first quintile being the one that groups the poorest population (154). On the other hand, the monetary poverty map can be estimated thanks to the national household survey (enaho) that allows obtaining an estimate of income and expenses of Peruvian households (156).
The sample for the determination of Hb upon admission to hospitalization was obtained by venipuncture. All Hb blood analyzes were processed in the sysmex model xn-1000 hematology analyzer, using the cyanide-free sodium lauryl sulfate (sls) methodology. Additionally, the analytical methodology had interlaboratory and external evaluation programs that ensured the quality of the results issued.
Statistical analysis
Statistical analyzes were performed using the statistical package for social science (spss, inc.) Software, version 26.0, which was also used for data management and cleaning. Descriptive statistics were reported as numbers and percentages for categorical variables. The evaluation of the normal distribution of the numerical variables was carried out with the kolmogorov-smirnov test, the student's t-test, and anova were used to compare hospital hemoglobin between participants with different clinical epidemiological characteristics, for the bivariate analysis of the qualitative variables. The chi-square test was used and regarding the multivariate analysis, a logistic regression was performed to obtain the adjusted or. The significance level was set at p<0.05 for all statistical analyses.
Results
It was observed that the population of infants was mostly male, with 61.4%. The analyzed population consisted predominantly of 2-month-old boys and girls, with 29.2%. 79.8% correspond to metropolitan lima and callao districts, and 96.3% belong to the quintiles with the highest economic income. When observing the nutritional status at the hospitalization time, acute malnutrition was found in 5.6% and severe malnutrition in 3% of the cases.
Regarding malnutrition due to excess, 7.9% presented overweight compared to 6.4% of the cases that presented obesity. The mean Hb was 10.4 g/dl with a standard deviation (sd) of 2. The mean Hb to the epidemiological characteristics was similar; however, it could only be associated with the age variable, reaching mean values of 14.4 g/dl (sd=2.2) in children under 1 month of age and up to a mean of 9.6 g/dl in infants of 2 months (sd=1.3),table 1.
Table 1. Hospital hemoglobin among participants with different clinical characteristics epidemiological, INSN 2017.
| Variables | Total | Hemoglobin (g/dl) | P value | ||||||
| N | % | Media | Of | ||||||
| Total | 267 | 100,0 | 10,4 | 2,0 | |||||
| Sex | 0,023 | ||||||||
| Masculine | 164 | 61,4 | 10,2 | 1,7 | |||||
| Femenine | 103 | 38,6 | 10,7 | 2,3 | |||||
| Age | 0,000 | ||||||||
| < 1us | 18 | 6,7 | 14,4 | 2,2 | |||||
| 1 us | 67 | 25,1 | 10,8 | 1,5 | |||||
| 2 months | 78 | 29,2 | 9,6 | 1,3 | |||||
| 3 months | 40 | 15,0 | 9,7 | 1,7 | |||||
| 4 months | 36 | 13,5 | 10,2 | 1,8 | |||||
| 5 months | 28 | 10,5 | 10,2 | 1,9 | |||||
| Residence area | 0,75 | ||||||||
| Metropolitan lima and callao | 213 | 79,8 | 10,4 | 1,9 | |||||
| Rest of the country | 54 | 20,2 | 10,3 | 2,1 | |||||
| Wealth quintile | 0,680 | ||||||||
| Quintile 2 and 3 - lowest income | 10 | 3,7 | 10,0 | 3,0 | |||||
| Quintile 4 and 5 - higher income | 257 | 96,3 | 10,4 | 1,9 | |||||
| Birth weight | 0,335 | ||||||||
| Low birth weight (<2500 g) | 18 | 6,7 | 9,8 | 2,8 | |||||
| Normal birth weight (≥2500 g) | 249 | 93,3 | 10,4 | 1,9 | |||||
| Length at birth | 0,483 | ||||||||
| Short length at birth (<45.4 cm-female; ≥46.1 cm-male) | 28 | 10,5 | 10,1 | 2,4 | |||||
| Adequate length at birth (≥45.4 cm-female; ≥46.1 cm-male) | 239 | 89,5 | 10,4 | 1,9 | |||||
| Head circumference at birth | 0,952 | ||||||||
| Microcephaly risk (<2ds) | 12 | 4,5 | 9,3 | 1,7 | |||||
| Normal (+-2ds) | 208 | 77,9 | 10,4 | 2,0 | |||||
| Macrocephaly risk (>2ds) | 47 | 17,6 | 10,7 | 1,8 | |||||
| Delivery characteristics | 0,428 | ||||||||
| Eutocic | 142 | 53,2 | 10,5 | 2,3 | |||||
| Dystocia | 125 | 46,8 | 10,3 | 1,6 | |||||
| Nutritional status (deficit and excess) | 0,426 | ||||||||
| Obesity | 17 | 6,4 | 9,5 | 2,1 | |||||
| Overweight | 21 | 7,9 | 10,4 | 1,5 | |||||
| Normal | 206 | 77,2 | 10,4 | 1,9 | |||||
| Acute malnutrition | 15 | 5,6 | 10,5 | 2,7 | |||||
| Severe malnutrition | 8 | 3,0 | 10,5 | 3,5 | |||||
When making the association between the presence of anemia in infants with the clinical and epidemiological variables (table 2), no association could be found with the parameters weight, length, head circumference, delivery characteristics, sex, origin, poverty quintile, hospital stay, and weight-for-age and length-for-age nutritional status. However, statistically significant associations were found in 3 different parameters: age, nutritional status, weight for length, and causes of hospitalization.
Table 2. Association between Hb level and clinical-epidemiological characteristics of hospitalized children under 6 months of age, INSN 2017.
| Variables | Hb blood levels in infants | P value | |||
| Anemia | Well, anemia | ||||
| N | % | N | % | ||
| Total | 178 | 66,7 | 89 | 33,3 | |
| Birth weight | |||||
| Low birth weight (<2500 g) | 11 | 61,1 | 7 | 38,9 | 0,605 |
| Normal weight at nacer (≥2500 g) | 167 | 67,1 | 82 | 32,9 | |
| Length at birth | |||||
| Short length at birth (<45.4 cm-female; <46.1 cm-male) | 18 | 64,3 | 10 | 35,7 | 0,778 |
| Adequate length at birth (≥45.4 cm-female; ≥46.1 cm-male) | 160 | 66,9 | 79 | 33,1 | |
| Head circumference at birth | |||||
| Microcephaly | 9 | 75,0 | 3 | 25,0 | 0,531 |
| Normal | 138 | 66,3 | 70 | 33,7 | 0,835 |
| Macrocephaly | 31 | 66,0 | 16 | 34,0 | 0,910 |
| Delivery characteristics | |||||
| Dystocia | 86 | 68,8 | 39 | 31,2 | 0,488 |
| Eutocic | 92 | 64,8 | 50 | 35,2 | |
| Sex | |||||
| Masculine | 116 | 70,7 | 48 | 29,3 | 0,075 |
| Femenine | 62 | 60,2 | 41 | 39,8 | |
| Origin | |||||
| Callao | 2 | 50,0 | 2 | 50,0 | 0,476 |
| Metropolitan lima1/ | 143 | 68,4 | 66 | 31,6 | 0,248 |
| Lima provincias2/ | 5 | 55,6 | 4 | 44,4 | 0,472 |
| Rest of country | 28 | 62,2 | 17 | 37,8 | 0,488 |
| Poverty quintile | |||||
| Quintile 2 | 2 | 100,0 | 0 | 0,0 | 0,315 |
| Quintile 3 | 3 | 37,5 | 5 | 62,5 | 0,076 |
| Quintile 4 | 64 | 64,6 | 35 | 35,4 | 0,052 |
| Quintile 5 | 109 | 69,0 | 49 | 31,0 | 0,591 |
| Age | |||||
| <1 month | 1 | 5,6 | 17 | 94,4 | 0,000 |
| 1 month | 39 | 58,2 | 28 | 41,8 | 0,090 |
| 2 months | 65 | 83,3 | 13 | 16,7 | 0,000 |
| 3 months | 32 | 80,0 | 8 | 20,0 | 0,052 |
| 4 months | 24 | 66,7 | 12 | 33,3 | 1,000 |
| 5 months | 17 | 60,7 | 11 | 39,3 | 0,480 |
| Nutritional status- weight for age | |||||
| Normal | 132 | 64,7 | 72 | 35,3 | 0,221 |
| Overweight | 31 | 79,5 | 8 | 20,5 | 0,066 |
| Under weight | 15 | 62,5 | 9 | 37,5 | 0,650 |
| Nutritional status - weight for length | |||||
| Over weight | 29 | 76,3 | 9 | 23,7 | 0,173 |
| Normal | 138 | 67,0 | 68 | 33,0 | 0,837 |
| Acute malnutrition | 11 | 47,8 | 12 | 52,2 | 0,045 |
| Nutritional status - length for age | |||||
| Normal | 161 | 66,0 | 83 | 34,0 | 0,441 |
| Low stature | 17 | 73,9 | 6 | 26,1 | |
| Causes of hospitalization (icd-10) | |||||
| Acute bronchiolitis (j21) | 52 | 73,2 | 19 | 26,8 | 0,170 |
| Whooping cough (a37) | 24 | 63,2 | 14 | 36,8 | 0,620 |
| Intestinal infections (a09) | 10 | 66,7 | 5 | 33,3 | 1,000 |
| Septicemia (a41) | 6 | 60,0 | 4 | 40,0 | 0,649 |
| Pneumonia (j15-j18) | 19 | 86,4 | 3 | 13,6 | 0,041 |
| Urinary tract infection (n39) | 8 | 80,0 | 2 | 20,0 | 0,362 |
| Conditions of perinatal origin (p00) | 0 | 0,0 | 8 | 100,0 | 0,000 |
| Blood volume depletion (e86) | 3 | 75,0 | 1 | 25,0 | 0,722 |
| Epilepsy (g40) | 9 | 56,3 | 7 | 43,8 | 0,362 |
| Other causes of hospitalization | 47 | 64,4 | 26 | 35,6 | 0,627 |
| Hospital stay | |||||
| 0 a 4 | 68 | 66,7 | 34 | 33,3 | 1,000 |
| 5 a 9 | 77 | 68,1 | 36 | 31,9 | 0,661 |
| 10 a 14 | 25 | 69,4 | 11 | 30,6 | 0,704 |
| 15 and over | 8 | 50,0 | 8 | 50,0 | 0,145 |
Regarding age, an association was only found with children under 1 month and 2 months; with nutritional status, only those who presented acute malnutrition; and with the causes of hospitalization, pneumonia, and conditions of perinatal origin.
It is important to highlight that anemia levels progressively increase to 83.3% in the second month of life, decreasing to 60.7% in the fifth month. Although there is no obvious association, it should be noted that 70.7% of men have anemia, 10% higher than women, and the 2 cases of the poorest quintile have anemia. Infants with excess weight present approximately a 10% increase in the level of anemia in relation to those classified with normal nutritional status, a progressive decrease in anemia levels is evident with longer hospitalization (table 2).
When performing a multivariate analysis between the median Hb (10.1 g/dl) and clinical-epidemiological factors (table 3), it was only possible to determine a statistically significant relationship (p<0.05) between Hb levels with the age of infants and that age progress increases by 3.8 if Hb levels drop. Although another multivariate association could not be determined, it can be established that a short length at birth increases the chances by 2.2 of presenting lower Hb levels.
Table 3. Multivariate analysis of Hb levels in hospitalized children under 6 months of age, INSN 2017.
| Variables | Probability Hb levels | P value | Adjusted or | Ic 95% | ||||||
| Hb≤10,1 g/dl | Hb>10.1 g/dl | |||||||||
| N | % | N | % | That | Ls | |||||
| Total | 139 | 100,0 | 128 | 100,0 | ||||||
| Birth weight | Low birth weight (<2500 g) | 10 | 7,2 | 8 | 6,3 | 0,4 | 0,5 | 0,1 | 2,3 | |
| Normal birth weight (≥2500 g) | 129 | 92,8 | 120 | 93,8 | ||||||
| Length at birth | Short length at birth (<45.4 cm-female; <46.1 cm-male) | 13 | 9,4 | 15 | 11,7 | 0,2 | 2,2 | 0,7 | 7,2 | |
| Adequate length at birth (≥45.4 cm-female; ≥46.1 cm-male) | 126 | 90,6 | 113 | 88,3 | ||||||
| Head circumference at birth | Risk | 32 | 23,0 | 27 | 21,1 | 0,1 | 0,6 | 0,3 | 1,1 | |
| Normal (+-2ds) | 107 | 77,0 | 101 | 78,9 | ||||||
| Delivery characteristics | Dystocia | 64 | 46,0 | 61 | 47,7 | 0,6 | 1,1 | 0,7 | 1,9 | |
| Eutocic | 75 | 54,0 | 67 | 52,3 | ||||||
| Sex | Masculine | 91 | 65,5 | 73 | 57,0 | 0,2 | 0,7 | 0,4 | 1,2 | |
| Femenine | 48 | 34,5 | 55 | 43,0 | ||||||
| Age | 0 to 1 my | 28 | 20,1 | 57 | 44,5 | 0,000 | 3,8 | 2,1 | 6,9 | |
| 2 to 5 months | 111 | 79,9 | 71 | 55,5 | ||||||
| Hospital stay | 0 to 6 days | 86 | 61,9 | 72 | 56,3 | 0,3 | 0,8 | 0,4 | 1,3 | |
| 7 or more days | 53 | 38,1 | 56 | 43,8 | ||||||
| Origin | Metropolitan lima and callao | 110 | 79,1 | 103 | 80,5 | 0,5 | 1,3 | 0,6 | 2,6 | |
| Rest of the country | 29 | 20,9 | 25 | 19,5 | ||||||
| Quintile | Quintile 2 and 3 - less income | 5 | 3,6 | 5 | 3,9 | 0,6 | 1,5 | 0,3 | 6,3 | |
| Quintile 4 and 5 - higher income | 134 | 96,4 | 123 | 96,1 | ||||||
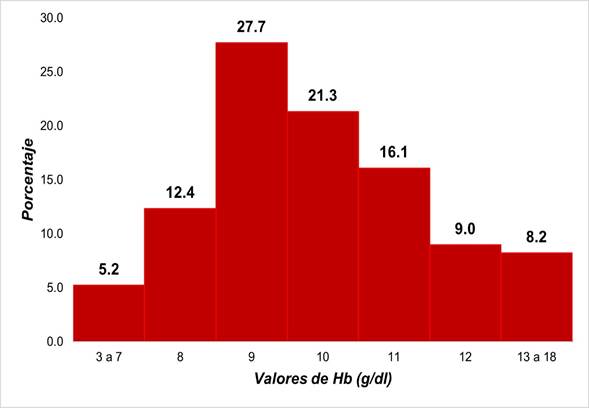
Infigure 2, it can be verified that the Hb levels concerning the percentage of the infant population. It is observed that 65.1% present an average Hb between the values of 9 to 11 g/dl.
Discussion
The results of this investigation are important because they allow associating clinical-epidemiological factors with anemia, especially at an early age; considering that the level of anemia in hospitalized children is usually 55%17or reaches values of 66.7% as in this investigation. In this first stage of life, one of the most common anemias occurs in neonates, known as physiological anemia. This occurs due to the progressive decrease in erythropoiesis that occurs from birth and reaches a peak between weeks 6 and 9.18
Internationally; it has been seen that the prevalence of anemia in this age group is slightly below that found in the present study. In nepal, a prevalence of 49% was found in children under 2 to 6 months of age.19; in a study from argentina carried out on children from 4 to 5 months, 28.9%20; and in another in brazil carried out on children from 3 to 5 months, 20.2%21.
Regarding age, an association was found between anemia and children in their first month and 2 months of life in the bivariate analysis and a lower median Hb in infants from 2 to 5 months in the multivariate analysis. Some studies associate changes in hemoglobin with the increasing age of the infant, up to 18 and 12 months, respectively, with the presence of anemia.2,22. Although this research worked with children under 6 months of age, the decrease in Hb levels due to the previously mentioned physiological anemia could still be extrapolated.18. On the other hand, infants, despite being hospitalized, present a decrease within what was expected in Hb levels given from month 1 to month 5. These results are similar to other studies in hospitalized infants in lebanon and turkey, where they observed that younger age of newborn hemoglobin levels23and ferritin24are older.
Another significant association found in this study, according to the bivariate analysis, was the causes of hospitalization. Only 2 complications that presented statistically representative associations with anemia could be determined: pneumonia and perinatal conditions. Previously published research has found an association between respiratory infections and anemia25,26; in this case, similar results were found, specifically with pneumonia. It should be noted that respiratory conditions are the most common cause of hospitalization in children17,27. Therefore, evaluating the repercussions of this association could be vital to grant better treatment.
In the same way, perinatal conditions have already been associated in previous studies with childhood anemia.28,30, which in turn has been seen to be the cause of abnormal neurological development if children have severe anemia due to the constant hypoxia to which they are subjected31.
Acute malnutrition, due to low weight for height, was another statistically associated variable in the bivariate analysis. Some studies on children under 1 year of age in asia have reached this same association.23,32; in addition, in the first of these, carried out specifically on the island of sri lanka, it was concluded that anemia has a greater association with acute malnutrition when hospitalized infants are younger and decreases concerning the age of the children.32.
The prevalence of anemia with hospital stay is another clinical-epidemiological factor that could not be associated in this investigation. This differs from the lebanese study carried out on children older than 6 months, where a statistically significant association was found with the presence of anemia, but from the fifth day of hospitalization23. Also, a second study conducted in adults associated an increase in hospital stay with the presence of any degree of preoperative anemia.33. It should be considered that a possible cause of this non-association in the present study may be due to the age difference of the patients in the two mentioned cases.
It should be considered that finding patients with anemia is recurrent in the hospitalization area17,34, and some investigations associate it with an increase in hospital mortality35,36. In addition, it has already been determined by other studies that this condition could aggravate the outcome of other diseases.35,36. For this reason, further research to relate this variable to anemia should be considered.
One limitation of the study was not having evaluated the parents' educational level, since in various investigations, it has been possible to determine a quite significant inverse association with the presence of anemia.2,3,5-8,17. Despite this, apart from the study carried out at the INSN in 201517, the associations were made in infants from 6 months of age and under 5 years.
Although in this investigation, no association was found between the level of wealth and the presence of anemia, the 2 infants who were within the second quintile of poverty were anemic; which can be compared to a study from tanzania that associated parental unemployment with the presence of anemia in hospitalized children under 5 years of age.37. Likewise, it has been seen in various studies carried out nationally and internationally, that the socioeconomic level does greatly influence the presence of this disease.9,10.
It is recommended to continue investigating the characteristics of anemia in the first months of life, in order to ensure a decrease in intrahospital mortality and have more tools against the fight against childhood anemia in Peru.
Conclusion
In conclusion, according to the bivariate analysis, a statistically significant association was found between age, acute malnutrition and causes of hospitalization and the presence of anemia; and regarding the multivariate analysis, it was possible to associate the median of the Hb levels with the age of boys and girls from 0 to 5 months of age hospitalized in the INSN.
REFERENCES
1. Irwin j, kirchner j. Anemia in children. Am fam physician. 2001;64(8):1379-86.disponible en: https://www.dilemata.net/revista/index.php/dilemata/article/view/369 [ Links ]
2. Neuman n, tanaka o, szarfarc s, guimarães p, victora c. Prevalência e fatores de risco para anemia no sul do brasil. Rev saude publica. 2000;34(1):56-63. Disponible en: https://revistasanitariadeinvestigacion.com/la-episiotomia-relacion-con-la-dispareunia-incontinencias-y-el-dolor-postparto-revision-bibliografica/ [ Links ]
3. Shamah-levy t, méndez-gómez-humarán i, gaona-pineda e, cuevas-nasu l, villalpando s. Food assistance programmes are indirectly associated with anaemia status in children <5 years old in mexico. Br j nutr. 2016;116(6):1095-102. Disponible en: http://dx.doi.org/10.4067/s0718-40262011000300016 [ Links ]
4. Khan j, islam m, biswas r, sultana a. An assessment of anemia status of child-mother pairs in bangladesh. Child youth serv rev. 2020;112:104851. Disponible en: https://www.thelancet.com/journals/lanwpc/article/piis2666-6065(21)00254-6/fulltext#seccesectitle0009 [ Links ]
5. Islam g. Association of socioeconomic status with childhood anemia among infant, toddler, and preschool children in bangladesh. Value heal reg issues. 2020;21:141-8. Disponible en: https://doi.org/10.18273/revsal.v50n4-2018005 [ Links ]
6. Afroja s, kabir r, islam a. Analysis of determinants of severity levels of childhood anemia in bangladesh using a proportional odds model. Clin epidemiol glob heal. 2020;8(1):175-80. Disponible en: https://www.thelancet.com/journals/lanwpc/article/piis2666-6065(21)00254-6/fulltext#tbl0002 [ Links ]
7. Sharma h, singh s, srivastava s. Socio-economic inequality and spatial heterogeneity in anaemia among children in india: evidence from nfhs-4 (2015-16). Clin epidemiol glob heal. 2020;8(4):1158-71. Disponible en: https://www.utic.edu.py/investigacion/index.php/reglamentos/codigo-de-etica-de-investigacion-cientifica-y-tecnologica [ Links ]
8. Dutta m, bhise m, prashad l, chaurasia h, debnath p. Prevalence and risk factors of anemia among children 6-59 months in india: a multilevel analysis. Clin epidemiol glob heal.2020;8(3):868-78. Disponible en: http://repositorio.upsjb.edu.pe/handle/upsjb/2090 [ Links ]
9. Águila-villar c, chávez-tejada e, romero-guzmán a, román-blas z, núñez-almache o. Anemia en la población pediátrica del Perú. Rev. Fac. Med. Hum. 2016;16(2):72-75. [ Links ]
10. velásquez-hurtado j, rodríguez y, gonzáles m, astete-robilliard l, loyola-romaní j, vigo we, et al. Factores asociados con la anemia en niños menores de tres años en Perú: análisis de la encuesta demográfica y de salud familiar, 2007-2013. Biomedica. 2016;36(2):220-9. Disponible en: http://www.scielo.org.co/pdf/rmri/v25n1/0122-0667-rmri-25-01-40.pdf [ Links ]
11. Instituto nacional de estadística e informática. Encuesta demográfica y de salud familiar-endes 2019 [internet]. [citado en sep 7 2020]. Disponible en: https://www.inei.gob.pe/media/menurecursivo/publicaciones_digitales/est/endes2019/ [ Links ]
12. Gomila a, de grandis e, visconti g, montero s, bertero m, marietti g, et al. Estado nutricional en niños internados en salas de cuidados mínimos. Hospital de niños de la santísima trinidad. Córdoba. Arch argent pediatr. 2009;107(1):37-42. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
13. Lopez a, cacoub p, macdougall i, peyrin-biroulet l. Iron deficiency anaemia. Lancet. 2016;387(10021):907-16. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
14. Instituto nacional de estadística e informática. La pobreza medida por quintiles de ingresos [internet]. [citado en sep 7 2020]. Disponible en: https://www.inei.gob.pe/media/menurecursivo/publicaciones_digitales/est/lib0386/cap0505.html [ Links ]
15. Instituto nacional de estadística e informática. Mapa de pobreza monetaria provincial y distrital 2018 [internet]. 2018 [citado en agos 8]. Disponible en: https://www.inei.gob.pe/media/menurecursivo/publicaciones_digitales/est/lib1718/libro.pdf [ Links ]
16. Ministerio de salud del Perú. Resolución ministerial n° 250-2017 [internet]. Apr 12, 2017. Disponible en: https://anemia.ins.gob.pe/sites/default/files/2017-08/rm_250-2017-minsa.pdf [ Links ]
17. Fernández-oliva j, mamani-urrutia v. Niveles de hemoglobina de lactantes de 0 a 6 meses de edad hospitalizados en el instituto nacional de salud del niño, 2015. An la fac med. 2019;80(1):45-50. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
18. Gkling p, schmidt r, roberts r, widness j. Serum erythropoietin levels during infancy: associations with erythropoiesis. J pediatr. 1996;128(6):791-6. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
19. Chandyo r, henjum s, ulak m, thorne-lyman a, ulvik r, shrestha p, et al. The prevalence of anemia and iron deficiency is more common in breastfed infants than their mothers in bhaktapur, nepal. Eur j clin nutr. 2016;70(4):456-62. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
20. Ianicelli j, barea a, falivene m, disalvo. L, apezteguía m, gonzález h. Prevalencia de anemia en lactantes menores de 6 meses asistidos en un centro de atención primaria de la ciudad de la plata. Arch argent pediatr. 2012;110(2):120-5. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
21. Guerreiro m, spanó a, aparecida i, azevedo f, bistafa m. La prevalencia de anemia en niños de 3 a 12 meses de vida en un servicio de salud de ribeirão preto, sp, brasil. Rev latino-am enferm. 2010;18(4). Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
22. Demirchyan a, petrosyan v, sargsyan v, hekimian k. Prevalence and determinants of anaemia among children aged 0-59 months in a rural region of armenia: a case-control study. Public health nutr. 2016;19(7):1260-9. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
23. Salami a, bahmad h, ghssein g, salloum l, fakih h. Prevalence of anemia among lebanese hospitalized children: risk and protective factors. Plos one. 2018;13(8):1-11. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
24. Altuntas n, beken s, kulali f, kazanci e, unal s, turan o, et al. Prevalence of iron deficiency at the first age of the infants hospitalized in neonatal period. Transfus apher sci 2012;47(1):85-9. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
25. Prentice a, bah a, jallow m, jallow a, sanyang s, sise e, et al. Respiratory infections drive hepcidin-mediated blockade of iron absorption leading to iron deficiency anemia in african children. Sci adv. 2019;5(3):1-8. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
26. Muthusamy b, venugopal v, sumithra s. Prevalence of anaemia among the hospitalized children in a rural tertiary care teaching hospital. Int j contemp pediatr. 2017;4(2):431. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
27. Gvelandia s, hodgson m, le roy c. Evaluación nutricional en niños hospitalizados en un servicio de pediatría. Rev chil pediatr. 2016;87(5):359-65. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
28. Radlowski e, johnson r. Perinatal iron deficiency and neurocognitive development. Front hum neurosci. 2013;7(585):1-11. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
29. Abu-ouf n, jan m. The impact of maternal iron deficiency and iron deficiency anemia on child's health. Saudi med j. 2015;36(2):146-9. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
30. Kalteren w, ter horst h, den heijer a, de vetten l, kooi e, bos a. Perinatal anemia is associated with neonatal and neurodevelopmental outcomes in infants with moderate to severe perinatal asphyxia. Neonatology. 2018;114(4):315-22. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
31. Kadooka m, kato h, kato a, ibara s, minakami h, maruyama y. Effect of neonatal hemoglobin concentration on long-term outcome of infants affected by fetomaternal hemorrhage. Early hum dev. 2014;90(9):431-4. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
32. keerthiwansa j, gajealan s, sivaraja s, subashini k. Malnutrition and anaemia among hospitalised children in vavuniya. Ceylon med j. 2014;59(4):141-3. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
33. Khanna r, harris d, mcdevitt j, fessler r, carabini l, lam s, et al. Impact of anemia and transfusion on readmission and length of stay after spinal surgery: a single-center study of 1187 operations. Clin spine surg . 2017;30(10):e1338-42. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
34. Wilson c, grant c, wall c. Iron deficiency anaemia and adverse dietary habits in hospitalised children. N z med j. 1999;112:203-6. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
35. vallejo c, correa f, solarte h, solano a, paz p, fajardo l, et al. Prevalencia de anemia en pacientes hospitalizados en el hospital universitario san josé de popayán. Repert med y cirugía. 2017;26(1):17-21. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
36. Velescu a, clará a, cladellas m, peñafiel j, mateos e, ibañez s, et al. Anemia increases mortality after open or endovascular treatment in patients with critical limb ischemia: a retrospective analysis. Eur j vasc endovasc surg. 2016;51(4):543-9. Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
37. Simbauranga r, kamugisha e, hokororo a, kidenya b, makani j. Prevalence and factors associated with severe anaemia amongst under-five children hospitalized at bugando medical centre, mwanza, tanzania. Bmc hematol. 2015;15(13). Disponible en: https://doi.org/10.1136/bmjopen-2020-043596 [ Links ]
8Article published by the journal of the faculty of human medicine of the ricardo palma university. It is an open access article, distributed under the terms of the creatvie commons license: creative commons attribution 4.0 international, cc by 4.0(https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: July 23, 2022; Accepted: December 19, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
