










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.23 no.1 Lima jan./mar. 2023 Epub 25-Jan-2023
http://dx.doi.org/10.25176/rfmh.v23i1.5061
Case Report
Ghost Cell Glaucoma: Clinical Case
1Servicio de Oftalmología, Hospital Nacional Carlos Alberto Seguín Escobedo - EsSalud. Arequipa, Peru.
2Facultad de Medicina Humana, Universidad Nacional de San Agustín. Arequipa, Peru.
3Facultad de Medicina Humana, Universidad Nacional Mayor de San Marcos. Lima, Peru.
Introduction:
Ghost cell glaucoma (GCG) is a rare secondary open angle glaucoma, in which there is a sustained increase in intraocular pressure (IOP) due to obstruction of the trabecular meshwork (TM) due to the passage of ghost cells (GC) from the vitreous into the anterior chamber, after a vitreous hemorrhage (VH).
Clinical Case:
We present the case of a male patient with a history of vitreous hemorrhage and sustained IOP elevation in the right eye (RE). Medical treatment was insufficient, for this reason surgical treatment was required. Postoperative evolution was advantageous.
Conclusion:
This pathology should prefer the differential diagnosis of traumatic glaucomas, correlating high clinical suspicion and histological confirmation.
Keywords: Glaucoma; ghost cells; intraocular pressure (Source: MeSH - NLM).
INTRODUCTION
Ghost cell glaucoma (GCF) is a secondary open-angle glaucoma that occurs after a long-lasting vitreous hemorrhage (VH), in which erythrocytes in the process of degeneration called "ghost cells" (GC) participate, which pass into the anterior chamber (AC) obstructing the trabecular meshwork (TM) and with it the flow of aqueous humor drainage, raising intraocular pressure (IOP)1.
Since its first description by Campbell and his collaborators in 1976, Ghost Cell Glaucoma (GCF) has been related to multiple processes of variable etiology, including traumatic and surgical events (pars plana vitrectomy, cataract extraction), metabolic, pharmacological, toxic (snake bite) and even spontaneous2.
It is a relatively infrequent disease at present, there have been few cases and series published regarding this pathology, making it difficult to obtain data on the prevalence and incidence of this disease3,4.
The diagnosis is clinical with histological confirmation in aqueous or vitreous humor, where it is possible to visualize GC under hematoxylin-eosin staining. In the differential diagnosis, hemolytic glaucoma, siderotic and hemosiderotic glaucoma, which are less frequent, must also be excluded, as well as avoiding confusion with neovascular glaucoma, uveitic glaucoma and endophthalmitis1,5.
The primary objective of the treatment consists of a correct management of IOP, to avoid damage to the optic nerve and the visual field. If there is refractory to medical treatment with ocular hypotensive drugs, surgical treatment should be considered. Within surgical treatment there are various therapeutic options such as anterior chamber lavage and pars plana vitrectomy; For glaucoma refractory to medical treatment due to chronic obstruction of the trabecular meshwork by GC, trabeculectomy or implantation of valved or non-valved drainage devices can be considered1,2,6.
We present the case of a male patient diagnosed with GCF. We emphasize the clinical presentation and cytological confirmation of this disease and the importance of being considered in the differential diagnosis of traumatic glaucomas.
CLINICAL CASE
We present the case of a 49-year-old man, who attended due to decreased visual acuity and pain in the right eye (RE). He refers a history of Type II Diabetes mellitus under treatment and an episode of ocular trauma due to the impact of a soccer ball on his RE approximately 2 months ago.
On the ophthalmological examination of the RE, he presented a better corrected visual acuity (BCVA) of counting fingers at a distance of 1 meter. The IOP was 40 mmHg. Slit-lamp examination of the anterior segment showed 1+ corneal edema, mild conjunctival hyperemia, formed anterior chamber, 3+ Tyndall's blood count (Figure 1).

Figure 1 Biomicroscopy of the anterior segment of the RE. Presence of hematic Tyndall 3+, formed anterior chamber. (Source: Clinical history)
The gonioscopy was normal. The eye fundus examination revealed a cloudy vitreous, unable to describe details of the papilla or the macula. The ophthalmological examination of the contralateral eye was normal.
Due to the clinical manifestations, it was decided to perform an anterior segment optical coherence tomography (OCT - SA) of the RE, where the anterior chamber was observed with punctate cellularity, of moderate density (Figure 2).
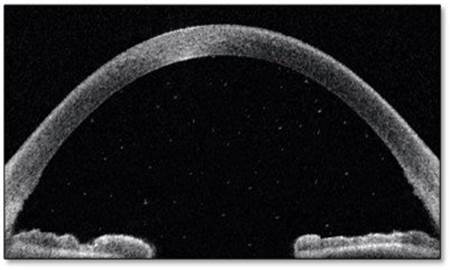
Figure 2 OCT-SA of the RE. Presence of punctate cellularity of moderate density in the anterior chamber. (Source: Clinical history)
Subsequently, a B-mode ultrasound of the RE is performed, where a diffuse increase in echogenicity is evident, compatible with vitreous hemorrhage; the retina was applied in the four quadrants (Figure 3).
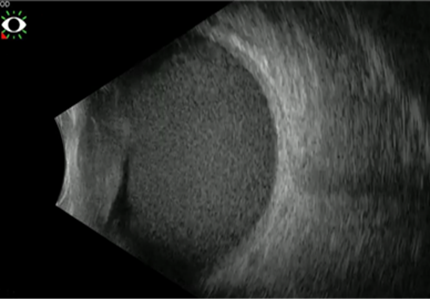
Figure 3 B-mode ultrasound of the RE. Diffuse increase in echogenicity, consistent with vitreous hemorrhage. (Source: Clinical History)
Paracentesis is performed to obtain a sample of aqueous humor and staining with hematoxylin-eosin is performed, evidencing the presence of spherical erythrocytes with traces of degenerated hemoglobin (Heinz bodies) (Figure 4).
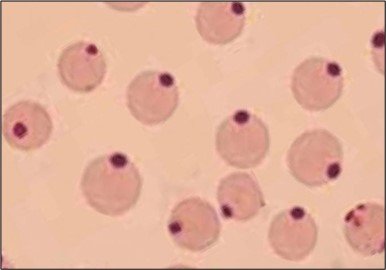
Figure 4 Histology of the aqueous humor of the RE. Presence of Heinz bodies. (Source: Clinical history)
For all of the above, the diagnosis of ghost cell glaucoma (GCF) is made and topical medical treatment is started with Timolol (0.5%) 1 drop every 12 hours, Dorzolamide (2%) 1 drop every 12 hours, Brimonidine (2 % ). 1 drop every 8 hours and Acetazolamide 250mg every 8 hours orally. It is reassessed later and persistence of elevated IOP is evident. Due to the evolution of the disease and the refractoriness to medical treatment, it was decided to opt for surgical treatment. In the RE, pars plana vitrectomy + anterior chamber lavage + non-valvular Baerveldt drainage implant was performed.
In the postoperative period, IOP remained within normal ranges. Two months after surgical treatment, an IOP of 15 mmHg and a BCVA of 20/70 were obtained, with clinical resolution of the ocular symptoms in the RE.
DISCUSSION
Ghost cell glaucoma (GCF) is a rare form of secondary open-angle glaucoma associated with degenerated erythrocytes (ghost cells), after prolonged vitreous hemorrhage, phantom cells develop in the vitreous and subsequently migrate to the anterior chamber to through the broken anterior hyaloid. As red blood cells degenerate in the vitreous, they change from their typical biconvex shape to khaki spherical ghost cells (erythroclasts). The latter are stiffer than normal erythrocytes and less able to cross the trabecular meshwork7.
The onset of ghost cell glaucoma is usually 2 to 3 weeks after trauma, as it takes at least 1 to 2 weeks for red blood cells to degenerate into ghost cells. Glaucoma caused by CF is characterized by ocular pain, prolonged IOP elevation, decreased visual acuity, absence of keratic precipitates, open iridocorneal angle assessed by gonioscopy, presence of fine khaki cells in AC, may also be deposited as Khaki-colored pseudohypopion or on a persistent hyphema secondary to previous ocular trauma, generating a double-layered level of red color for fresh red blood cells, and khaki color corresponding to FC, which is known as the caramel stripe sign1,8,9.
In the present case there was refractoriness to medical treatment, for which reason surgical management was considered, performing a pars plana vitrectomy + anterior chamber lavage + implantation of a non-valved Baerveldt drainage device. The treatment was successful since IOP control was achieved.
CONCLUSIONS
GCF is a very rare disease, but it must be considered within the differential diagnosis of traumatic glaucoma. In the present case, the diagnosis was based on high clinical suspicion and histological confirmation. The GCF usually has a good response to medical treatment, but as observed in the present case, the IOP could not be controlled, for which surgical treatment was required, achieving a good clinical evolution after this.
REFERENCES
1. Álvarez E, Viera D, Galvan F, et al. Glaucoma de células fantasmas: revisión de la literatura. Arch Soc Canar Oftal. 2021; 32:129-134. Disponible en: https://sociedadcanariadeoftalmologia.com/wp-content/revista/revista-32/32sco22.pdf [ Links ]
2. Delgado S, Hernández A. Glaucoma de células fantasmas: Reporte de caso. Rev Medica MD. 2015;6(3):214-217. Disponible en: https://www.medigraphic.com/pdfs/revmed/md-2015/md153g.pdf [ Links ]
3. Lazo A. Glaucoma de células fantasmas secundario a Sindrome de Terson en un ojo fáquico. Alerta. 2021;4(3):92-97. DOI: https://doi.org/10.5377/alerta.v4i3.11131 [ Links ]
4. Frazer D, Kidd M, Johnston P. Ghost cell glaucoma in phakic eyes. Int Ophthalmol. 1987;11(1):51-54. DOI: https://doi.org/10.1007/BF020278971 [ Links ]
5. Cameron J, Havener V. Histologic confirmation of ghost cell glaucoma by routine light microscopy. Am J Ophthalmol. 1983;96(2): 251-252. DOI: https://doi.org/10.1016/S0002-9394(14)77797-9 [ Links ]
6. El-Asrar A, Al-Obeidan S. Pars plana vitrectomy in the management of ghost cell glaucoma. Int Ophthalmol. 1995;19:121-124. DOI: https://doi.org/10.1007/BF00133183 [ Links ]
7. Grupo de trabajo de la Guía de Práctica Clínica para Detección, Diagnóstico y Tratamiento del Glaucoma Traumático en el Instituto Nacional de Oftalmología - INO "Dr. Francisco Contreras Campos"; 2021. Disponible en: https://www.ino.gob.pe/wp-content/uploads/2021/11/RD_N_129_2021_INO_D.pdf (acceso 18 de julio del 2022) [ Links ]
8. Temblador I, Espejo A, López J, et al. Glaucoma por células fantasma. Actual Med. 2019;104(806):46-47. DOI: https://doi.org/10.15568/am.2019.806.cc01 [ Links ]
9. Campbell D. Ghost Cell Glaucoma Following Trauma. Am Acad Ophthalmol. 1981;88(11):1151-1158. DOI: https://doi.org/10.1016/S0161-6420(81)34892-1 [ Links ]
10. Alamri A, Alkatan H, Aljadaan I. Traumatic Ghost Cell Glaucoma with Successful Resolution of Corneal Blood Staining Following Pars Plana Vitrectomy. Middle East Afr J Ophthalmol. 2016;23(3):271-273. DOI: https://doi.org/10.4103/0974-9233.180778 [ Links ]
8 Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0(https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: June 22, 2022; Accepted: January 16, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
