










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.23 no.1 Lima ene./mar. 2023 Epub 25-Ene-2023
http://dx.doi.org/10.25176/rfmh.v23i1.5290
Case Report
Small bowel arteriovenous malformation as a cause of dark gastrointestinal bleeding: Two Instructional Cases
1Instituto de investigaciones en Ciencias Biomédicas, Universidad Ricardo Palma, Lima, Peru.
2Servicio de Patología quirúrgica, Hospital Edgardo Rebagliati Martins. Lima, Peru.
3Laboratorio Diagnosis S.A.C. Lima, Peru.
4Hospital Emergencia Ate-Vitarte. Lima, Peru.
5Centro de Salud Arcata, Gerencia Regional de Salud de Arequipa. Arequipa, Perú.
Introduction:
Digestive bleeding can put patients’ lives at risk, even more so when the origin is not located in routine upper and lower endoscopy. The small intestine is the largest portion of the digestive tract and being a source of bleeding means a diagnostic and therapeutic medical challenge.
Clinical case:
We presented cases of two female patients, 53 and 60 years old, who develop digestive bleeding, locating its origin in the small bowel and undergoing surgical removal of the affected intestinal segment. The anatomopathological study finds malformed arteries and veins that communicate without an intermediate capillary bed. The diagnosis was arteriovenous malformation, a rare entity in the small bowel. Both cases are reviewed with emphasis on the histopathological criteria and their clinical correlation.
Keywords: Arteriovenous malformation; small bowel; digestive bleeding (Source: MeSH NLM).
INTRODUCTION
Arteriovenous malformation (AVM) is characterized histopathologically by a conglomerate of blood vessels with abnormally formed walls that connect directly to each other, without a capillary bed between both types of vessels. They usually cause hemorrhage and are frequently located in the central nervous system, involvement of the small intestine being very unusual.
The term AVM implies the presence of an arterial feeder with an abrupt transition to the veins without an intermediate capillary bed. This characteristic is essential to differentiate it from angioectasias, venous lesions, and Dieulafoy lesions, which are arterial1.
Dark gastrointestinal bleeding has been defined as bleeding of unidentified origin that persists despite careful upper and lower endoscopic evaluation2. Although unobserved lesions in the esophagus, stomach, duodenum, and colon must be considered, most sources of bleeding are identified in the small intestine3, representing approximately 5% of all cases of gastrointestinal bleeding4.
Although routine endoscopic evaluation (upper and lower) is usually negative for small-bowel bleeding, the presence of blood in the terminal ileum is an independent risk factor indicative of a small-bowel origin5.
Although most of them are asymptomatic, they can manifest with intense abdominal pain or bleeding, and can occur at any age. Intestinal AVMs in adults usually involve the cecum and the right colon6. However, in children they frequently occur in the jejunum causing obstruction or intussusception7.
AVMs are usually large and susceptible to rebleeding, which is why they usually require surgical resection8.
AVMs of the digestive tract have been divided into three types by Moore's classification9. Those of type 1 are usually acquired, in elderly patients, affecting the ascending colon, small and hardly visible. Type 2 are usually congenital, in younger patients, affecting the small intestine, larger and more visible. Type 3 is hereditary, as in Rendu-Osler-Weber disease.
Intestinal AVMs can cause severe anemia and life-threatening bleeding, sometimes requiring emergency surgery10. Endoscopic clips or tattoos can help locate the affected small bowel segment during surgery11.
Considering that each patient has its own characteristics as a host of any disease, two clinical cases of particular interest are presented below.
DESCRIPTION OF CLINICAL CASES
Case 1. A 60-year-old woman, with a 5-year history of autoimmune hepatitis, who consulted due to paleness and fatigue. Laboratory tests detected a hemoglobin of 10.9 g/dL, a hematocrit of 35.7%, and a mean corpuscular volume of 83.8 fl. Upper and lower endoscopy was performed without finding major alterations, being programmed for retrograde enteroscopy due to suspicion of digestive bleeding, which was frustrating. Instead, they performed an endoscopic capsule test where an ill-defined subepithelial lesion was discovered. Subsequently, enteroscopy was performed, finding a lobulated, bluish lesion 3.8 meters from the angle of Treitz, measuring about 35mm, with oozing bleeding. Marking was done with black Chinese ink tattoo. Subsequently, during surgery, the lesion was confirmed, performing resection of a segment of the small intestine and release of omental adhesions.
In the pathology study, the macroscopy described a 10x1.5x1.5cm small intestine segment, congested serosa with a paracentral blackish area (tattoo). When the specimen was opened, a raised lesion was observed, measuring 12x8x4mm, grayish, elastic, and covered by mucosa with a normal appearance to the surrounding one (Figure 1A). On serial section, dilated irregular vessels were observed, located mainly in the submucosa, with a slight retraction of the muscle layer. Microscopically, the lesion corresponded to vascular tangles, with arteries and veins of various diameters, walls with structural alterations, and arteriovenous anastomoses, with no evident capillary bed (Figure 1C).
Histochemical staining for elastic fibers demonstrated multiple structural alterations (Figure 1E). The final diagnosis was arteriovenous malformation, predominantly in the submucosa of the small intestine. In subsequent medical check-ups, the patient did not present rebleeding or other significant changes.
Case 2. A 53-year-old woman with a history of hypothyroidism, who consulted due to loss of consciousness, paleness, and respiratory distress. Laboratory tests detected a hemoglobin of 7.1 g/dL, a hematocrit of 24.3, and a mean corpuscular volume of 87.1 fl. Upper and lower endoscopy was performed, finding elevated gastric lesions with a benign appearance and colonic diverticulosis without bleeding, respectively. Days later, they performed a capsule endoscopy test, which found diluted bleeding and the presence of a tapeworm that obstructed vision. She was hospitalized and received treatment for taeniasis. Subsequently, they performed an enteroscopy, which found a violaceous lesion in the middle jejunum associated with blood content from the distal middle jejunum. Tattoo was done with black Chinese ink. During surgery, a vascular lesion in the middle jejunum was described, associated with spider veins in the mesentery, and a segment of the small intestine was resected.
In the pathology study, the macroscopy described a 13x1.5x1.5cm segment of the small intestine, congested serosa with a paracentral blackish area (tattoo) and tortuous/congestive vessels were observed at the level of the mesenteric root (Figure 1B). When the specimen was opened, the mucosa was congestive and irregularly nodular in the area described, measuring 12x10mm, with no clear contours. On serial section, congestive and tortuous vessels were observed occupying almost the entire thickness of the intestinal wall.
Microscopically, vascular tangles were observed, with arteries and veins of different diameters, walls with structural alterations and arteriovenous anastomoses, without a capillary bed, which affected up to the subserosa (Figure 1D) and an identical focus was found in the mesentery. Histochemical staining for elastic fibers demonstrated their discontinuity and irregular thickness (Figure 1F). The final diagnosis was arteriovenous malformation, involving the submucosa, muscularis propria, subserosa, and mesenteric root of the small intestine. In subsequent medical check-ups, the patient did not present rebleeding or other significant alterations.
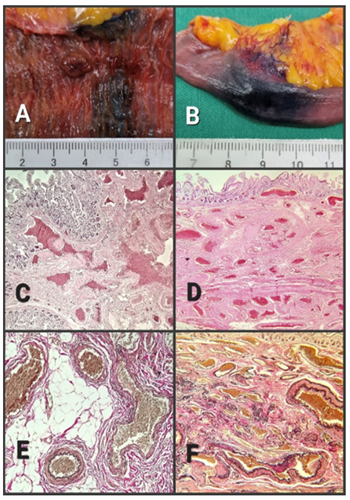
A. Case 1, The plateau-type submucosal lesion, adjacent to the tattoo área B. Case 2, vascular tangles visible from serosa to root of mesentery C. Case 1, vascular tangles with structural alterations in walls of arteries and veins without capillary bed, affecting submucosa (40X) D. Case 2, vascular tangles similar to the previous case affecting from submucosa to intestinal subserosa (40X) E. Case 1, staple elastic fibers in black color (100X) F. Case 2, staple elastic fibers in black color (100X)
DISCUSSION
AVM that affects the small intestine is very rare, and locating it in the jejunum-ileum, which measures about 6 meters, represents a medical challenge. Upper endoscopy allows a very precise evaluation from the esophagus to the duodenum. A similar situation occurs with lower endoscopy for evaluation from the anal canal to the distal ileum. Both studies do not allow an adequate evaluation of the jejunum-ileum, the largest portion of the digestive tract. There are other methods available such as enteroscopy and capsule endoscopy for such evaluation.
Gastrointestinal bleeding of obscure origin can risk the patient's life and represent a true medical emergency. In these cases, a rapid and targeted approach is required, considering that the sources of bleeding in the small intestine have peculiar characteristics and must be regarded as neoplastic and non-neoplastic lesions. It is known that primary adenocarcinomas of the small intestine are extremely rare, with neuroendocrine neoplasia being the most frequent. Among non-neoplastic lesions, vascular lesions should be considered, such as AVM and others.
Based on endoscopic findings, Yano et al.12classified vascular lesions of the small intestine into six groups. Types 1a (punctate erythema less than 1 mm) and 1b (patchy erythema) are venous or capillary lesions and are considered angioectasias. Type 2a (punctate lesion less than 1 mm with pulsatile bleeding) and 2b (pulsatile red protrusion without surrounding venous dilatation) are arterial lesions and are considered Dieulafoy lesions. Type 3 (pulsatile red protrusion with surrounding venous dilation) are AVMs. Type 4 corresponds to vascular lesions with unusual morphology and cannot be classified.
Clinically, it is useful to remember the semiology of gastrointestinal bleeding, where rectal bleeding is the presence of bright red blood originating from the rectum; hematochezia is blood mixed with feces, dark red and usually comes from the small or large intestine, while the melena is black digested blood originating proximally in the digestive tract.
The cases presented correspond to women aged 53 and 60, with non-digestive comorbidities and who present signs and symptoms associated with chronic blood loss. Directed studies find vascular-like lesions, both in the middle jejunum, one of them with oozing bleeding. On both occasions it was possible to make the tattoo with Chinese ink, to facilitate the location in the surgical act. Once the surgical resections were performed, the histopathological study with hematoxylin-eosin showed that both lesions corresponded to tangles of arterial and venous vessels, with architecturally altered walls, which communicated directly, without an intermediate capillary bed. In case 1, the lesion mainly affected the submucosa, while in case 2, almost the entire wall, including the root of the mesentery. The special staining for elastic fibers evidenced their multifocal discontinuity in the vascular walls. Both cases corresponded to type 2, according to Moore's classification, and type 3, according to Yano's endoscopic classification. The definitive anatomopathological diagnosis was arteriovenous malformation in the small intestine, a rare lesion.Table 1summarizes the main characteristics of both cases.
Table 1
| CASE 1 | CASE 2 | |
| Gender | Feminine | Feminine |
| Age | 60 | 53 |
| Pathological history | Autoimmune hepatitis | Hypothyroidism, taeniasis |
| Signs-symptoms | Paleness, tiredness distress | Loss of consciousness, paleness, respiratory distress |
| Hemoglobin value in g/dL | 10.9 | 7.1 |
| Capsule endoscopy | Yes | Yes |
| Enteroscopy | Yes | Yes |
| Tattoo with black Chinese ink | Yes | Yes |
| Surgery (exploratory laparotomy) | Yes | Yes |
| Lesion location | Middle jejunum | Middle jejunum |
| Lesion size | 12x8x4mm | 12x10mm |
| Shape of the lesion | On plateau | Diffuse, thickens the wall up to 5mm |
| Compromise of intestinal layers | Submucosa | Submucosa, muscularis propria, and subserosaa |
| Involvement of the mesentery | No | Yes |
| Postoperative evolution / controls | Favorable | Favorable |
CONCLUSION
AVM is considered a congenital vascular lesion, which can affect any body tissue, but is much more frequent in the central nervous system. The location in the digestive tract is infrequent and in the small intestine, even more infrequent. It usually causes chronic digestive bleeding, but also abrupt, putting the lives of patients at risk. Anemia in chronic cases is the rule and loss of consciousness is usually related to dangerous sudden and massive gastrointestinal bleeding.
A high degree of clinical suspicion and a defined protocol are required for the diagnostic approach to these lesions, which must culminate in the exact location and resection of the lesion, due to the high risk of rebleeding described. There are other therapeutic options, the utility and indication of which are beyond the scope of this publication.
The histopathological study must be thorough, from microscopy to the microscopic finding of structural alterations in vascular walls, and must be complemented with histochemical staining to demonstrate the alterations in the wall elastic fibers, characteristic of this lesion.
REFERENCES
1. Holleran G, Hall B, O'Regan M. Expression of Angiogenic Factors in Patients with Sporadic Small Bowel Angiodysplasia. J Clin Gastroenterol. 2015;49:831. DOI: https://doi.org/10.1097/MCG.0000000000000260 [ Links ]
2. ASGE Standards of Practice Committee; Gurudu SR, Bruining DH, Acosta RD, Eloubeidi MA, Faulx AL, Khashab MA, Kothari S, Lightdale JR, Muthusamy VR, Yang J, DeWitt JM. The role of endoscopy in the management of suspected small-bowel bleeding. Gastrointest Endosc 2017; 85: 22-31 [PMID:27374798] DOI: https://doi.org/10.1016/j.gie.2016.06.013 [ Links ]
3. 3 Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding. Am J Gastroenterol 2015; 110: 1265-87; quiz 1288 [PMID: 26303132] DOI: https://doi.org/10.1038/ajg.2015.246 [ Links ]
4. Lewis BS. Small intestinal bleeding. Gastroenterol Clin North Am 1994; 23: 67-91 [PMID: 8132301] DOI: https://doi.org/10.1016/S0889-8553(05)70108-4 [ Links ]
5. Micic D, GaetanoJN, Nigam N , Peller M , Rao VL, Semrad C , et al . Risk factors for small bowel bleeding in an overt gastrointestinal bleeding presentation after negative upper and lower endoscopy. PLoSOne2019;14:e0212509. DOI: https://doi.org/10.1371/journal.pone.0212509 [ Links ]
6. Lee HH, Kwon HM, Gil S, Kim YS, Cho M, Seo KJ, et al. Endoscopic resection of asymptomatic, colonic, polypoid arteriovenous malformations: two case reports and a literature review. Saudi J Gastroenterol 2017;23:67-70. DOI: https://doi.org/10.4103/1319-3767.199111 [ Links ]
7. Yazbeck N, Mahfouz I, Majdalani M, Tawil A, Farra C, Akel S. Intestinal polypoid arteriovenous malformation: unusual presentation in a child and review of the literature. Acta Paediatr 2011; 100:e141-4. DOI: https://doi.org/10.1111/j.1651-2227.2011.02203.x [ Links ]
8. Sakai E, Ohata K, Nakajima A, Matsuhashi N. Diagnosis and therapeutic strategies for small bowel vascular lesions. World J Gastroenterol. 2019 Jun 14;25(22):2720-2733. DOI: https://doi.org/10.3748/wjg.v25.i22.2720 [ Links ]
9. Moore JD, Thompson NW, Appleman HD, Foley D. Arteriovenous malformation of the gastrointestinal tract. Arch Surg. 1976; 111(4):381-9. DOI: https://doi.org/10.1001/archsurg.1976.01360220077013 [ Links ]
10. Small intestinal arteriovenous malformation treated by laparoscopic surgery using intravenous injection of ICG: Case report with literature review Takahiko Hyo, Kenji Matsuda, Koichi Tamura, Hiromitsu Iwamoto, Yasuyuki Mitani,Yuki Mizumoto, Yuki Nakamura, Hiroki Yamaue; International Journal of Surgery, Case Reports 74 (2020) 201-204. DOI: https://doi.org/10.1016/j.ijscr.2020.08.038 [ Links ]
11. Chung CS, Chen KC, Chou YH, Chen KH. Emergent single-balloon enteroscopy for overt bleeding of small intestinal vascular malformation. World J Gastroenterol. 2018;24:157-60. DOI: https://doi.org/10.3748/wjg.v24.i1.157 [ Links ]
12. Yano T, Yamamoto H, Sunada K, et al. Endoscopic classification of vascular lesions of the small intestine (with videos). Gastrointest Endosc 2008;67:169-172. https://doi.org/10.1016/j.gie.2007.08.005 [ Links ]
8 Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0(https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: October 28, 2022; Accepted: January 03, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
