










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versão impressa ISSN 1814-5469versão On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.23 no.3 Lima jul./set. 2023 Epub 21-Set-2023
http://dx.doi.org/10.25176/rfmh.v23i3.5659
Original Article
Emotional inteligence and stress coping strategies in health care workers
1Universidad Científica del Sur, Lima-Perú
2Latin American Lifestyle Medicine Association (LALMA)
Objective:
To determine the relationship between emotional intelligence and stress coping strategies in health care workers of a Third Level of Care Hospital during 2021.
Methods:
An analytical cross-sectional study was carried out. Two surveys were used: the COPE test which measures how to cope with stress and the Bar-On Emotional Coefficient Inventory which measures the level of emotional intelligence. The main variable was coping with stress. The independent variable was emotional intelligence.
Results:
A total of 290 health care workers were worked. Emotional intelligence was significantly positively correlated (Pearson = 0.6003) with stress coping. The stress coping strategies with the highest mean were planning, positive reinterpretation and growth, and religious coping. These strategies had a positive correlation with emotional intelligence, these correlations were 0.5271, 0.5200 and 0.2051 respectively. For the multiple regression analysis, it was observed that the average BARON test score increased by 0.261 points for each point increase in the COPE TEST (coefficient = 0.261; 95%CI: 0.215 - 0.307); adjusted for all covariates of interest.
Conclusion:
There is a relationship between emotional intelligence and stress coping. A relationship was also found with stress coping strategies.
Keywords: Emotional intelligence; coping; coping; stress; caregivers (Mesh Terms)
INTRODUCTION
Worldwide, occupational stress in developing countries represents approximately 5% to 10%, and in industrialized countries it increases approximately 20% to 50%.1In Latin America, several countries are affected, as is the case of Argentina, where it was found that 65% of workers in the Federal Capital suffer from occupational stress. In Mexico, work stress represents 75% of its workers, where the most stressful factor was the workload.1In Peru, 78% of workers suffer from work-related stress and 89% of them said that the companies where they worked did not have measures in place to avoid or reduce work-related stress.3
Emotional Intelligence (EI) is the ability that allows us to perceive, understand, assimilate and regulate emotions, it also promotes emotional self-control.1While, coping strategies are the cognitive and behavioral effort made to master external (environmental) or internal (emotional state) situations, they are evaluated as something that exceeds the person's resources.5Emotional intelligence is very important to opt for the best coping strategies in the face of stress, a very important soft skill in various types of workers, especially those who are exposed to a high stress load, as is the case of health personnel.6
The World Health Organization (WHO) emphasizes on work stress in health personnel, since they are more exposed to high levels of stress due to the demanding interaction with people suffering from any ailment.7)(8Knowing how stress affects and is managed in health personnel is important because stress can cause physical and psychological damage, which can lead to health personnel not being able to perform their duties adequately, affecting the quality of patient care and the productivity of health personnel.9Therefore, the objective of this study was to determine the relationship between emotional intelligence and stress coping strategies in health care workers of a Third Level of Care Hospital.
MATERIALS AND METHODS
Study population
The study population consisted of the health care personnel of the Hospital Arzobispo Loayza, Lima, Peru.
All subjects who participated in the study signed a consent form before being surveyed. The sample size was calculated for finite populations, since we had the population size (N=514), with an expected proportion of 0.5, confidence level of 95%, with an error of 0.05; from which a sample of 290 workers was obtained. The sample was selected by non-probabilistic convenience sampling.
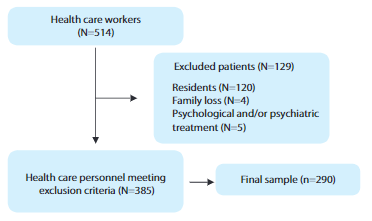
Elegibility criteria
In this study, only health care personnel appointed or under administrative service contract (CAS) were included. Health personnel who are in their residency and/or completing their training, health personnel who have had a recent family loss (6 months prior to the date of the health personnel survey) and personnel who are receiving psychological and/or psychiatric treatment were excluded.
Variables and measurement
Response variable
The Multidimensional Inventory of Coping Evaluation (COPE) test. It measures coping strategies and determines coping styles to stress.(10)The test is composed of 60 items, has a Likert-type format consisting of four alternatives ranging from 1 to 4; 1 = I almost never do this, 2 = Sometimes I do this, 3 = Usually I do this and 4 = I do this very often.(10)In addition, it has been used and validated in the Peruvian population.(10)The results are obtained by adding the scores according to the responses to each item, and this score obtained is divided by the number of items it has according to the dimension to which it belongs.
The test presents 15 strategies, which are: active coping, planning, containment of coping, suppression of activities, positive reinterpretation and growth, acceptance, focusing and releasing emotions, search for instrumental HH reasons, search for emotional HH reasons, mental disengagement, behavioral disengagement, denial, religious coping, use of humor and use of substances. It also presents 3 styles, models or factors, which would be: Task-Directed Coping Style, Social and Emotional Coping Style and Avoidant Coping Style.
Exposure variables
The BarOn Emotional Intelligence Inventory Test (EIT) evaluates the emotional aptitudes of the personality that influence the achievement of overall success and adequate emotional health.(11)This test is comprised of 133 items, has a Likert-type format consisting of four alternatives which range from 1 to 5; 1 = Rarely or never is my case, 2 = Rarely is my case, 3 = Sometimes is my case, 4 = Many times is my case and 5 = Very often or always is my case. In addition, it has been used and validated in the Peruvian population.(11)The results are obtained by adding the scores according to the answers of each item. The emotional coefficient scores can be categorized as high (> 100), medium (70-99) and low (25 to 69). The test presents 6 components; the Intrapersonal (IA), Interpersonal (IE), Adaptability (AD), Stress Management (ME), General Mood (AG), CE standard score of the I-CE. It also presents subcomponents, the intrapersonal subcomponent (self-understanding, assertiveness, self-concept, self-actualization, independence); interpersonal subcomponent (empathy, interpersonal relationships, social responsibility); adaptability subcomponents (problem solving, reality testing, flexibility); stress management subcomponent (stress tolerance, impulse control) and the general mood subcomponent (happiness, optimism).
Other variables
The variables were age; sex (male, female); marital status (single, cohabitant, separated, married, divorced); position (dentist, physician, nursing technician, nurse, technologist); type of contract (appointed, CAS); type of work (semi-presential, face-to-face).
Procedures
The researchers, with the prior permission of the institution, surveyed the health personnel virtually using a data collection form divided into 3 parts: the first part was sociodemographic data, the second part was the BarOn test, and the third part was the COPE test. All health personnel who met the inclusion criteria were surveyed.
Statistical analysis
Statistical analysis with STATA v17.0 software. For the descriptive analysis, the qualitative variables were summarized in percentages; while for the quantitative variable will be presented as mean and standard deviation. In the bivariate analysis, the Student's t-test and Mann-Whitney U test were used for dichotomous and numerical categorical variables, and the Kruskal Wallis test for polychotomous and numerical categorical variables. The Spearman test was also used for numerical variables.
We performed the multivariate generalized linear model of the Gaussian family from a linear regression model. The variables included in the multivariate model were age, sex, marital status, position, type of contract and type of work. These variables were chosen from the literature review. The measure of association was the beta coefficient with its respective 95% confidence interval (CI).
Ethical considerations
The present work was approved by the Hospital and the ethics committee of the Faculty of Medicine of the Southern Scientific University. The study participants gave their oral consent. In addition, all ethical research guidelines and the Declaration of Helsinki were respected.
RESULTS
A total of 290 health personnel were studied. The average age was 41 years, women were found to be the predominant sex (81.38%); being single was 41.385%, the predominant job position was nurse (50.34%), the majority type of contract was appointed (54.83%); and the predominant type of work was face-to-face (99.66%). The mean of the BARON test was 347.86 points and the mean of the COPE test was 138.84 points (Table 1).
Table 1. General characteristics of a sample of individuals
| Features | n % |
| Age | 41.4 (8.97)* |
| Sex | |
| Male | 54 (18.62) |
| Female | 236 (81.38) |
| Marital Status | |
| Single | 120 (41.38) |
| Cohabitant | 44 (15.17) |
| Separated | 116 (40.00) |
| Married | 8 (2.76) |
| Divorced | 2 (0.69) |
| Post | |
| Dentist | 1 (0.34) |
| Physitian | 37 (12.76) |
| Nursing technician | 96 (33.10) |
| Nurse | 146 (50.34) |
| Technologist | 10 (3.45) |
| Type of contract | |
| Named | 159 (54.83) |
| CAS | 131 (45.17) |
| Type of work | |
| Semi-attendance | 1 (0.34) |
| On-site | 289 (99.66) |
| BARON test | 347.86 (46.52) * |
| COPE test | 138.84 (22.31) * |
| COPE test strategies | |
| Religious coping | 12.05 (2.97) * |
| Positive reinterpretation and growth | 11.94 (2.49) * |
| Planning | 11.13 (2.69) * |
(*) mean and standard deviation
The components and subcomponents of the BARON test (emotional intelligence) are described. Of the components stress management had a high predominance (76.90%), and in the stress management subcomponent, impulse control had a predominance of 91.38% (Table 2).
Table 2. Components and subcomponents of emotional intelligence (BARON test) of the sample of individuals
| EMOTIONAL INTELLIGENCE | |||
|---|---|---|---|
| Under n(%) | Medium n(%) | High n(%) | |
| COMPONENTS | |||
| Intrapersonal (IA) | 13 (4.48) | 212 (73.10) | 65 (22.41) |
| Interpersonal (IE) | 91 (31.38) | 153 (52.76) | 46 (15.86) |
| Adaptability (AD) | 12 (4.14) | 208 (71.72) | 70 (24.14) |
| Stress Management (SM) | - | 67 (23.10) | 223 (76.90) |
| General Mood (GA) | 49 (16.90) | 171 (58.97) | 70 (24.14) |
| Score I-CE CE standard | 14 (4.83) | 190 (65.52) | 86 (29.66) |
| SUBCOMPONENTS | |||
| INTRAPERSONAL SUBCOMPONENT (IA) | |||
| Self-understanding (CM) | 4 (1.38) | 224 (77.24) | 62 (21.38) |
| Assertiveness (AS) | 37 (12.76) | 191 (65.86) | 62 (21.38) |
| Self-concept (AC) | 19 (6.55) | 194 (66.90) | 77 (26.55) |
| Self-actualization (AR) | 20 (6.90) | 203 (70.00) | 67 (23.10) |
| Independence (IN) | 37 (12.76) | 149 (51.38) | 104 (35.86) |
| INTERPERSONAL SUBCOMPONENT (IE) | |||
| Empathy (EM) | 143 (49.31) | 120 (41.38) | 27 (9.31) |
| Interpersonal Relations (IR) | 60 (20.69) | 179 (61.72) | 51 (17.59) |
| Social Responsibility (SR) | |||
| ADAPTABILITY SUBCOMPONENT (AD) | |||
| Troubleshooting (SP) | 52 (17.99) | 177 (61.25) | 60 (20.76) |
| Reality Test (PR) | 10 (3.45) | 213 (73.45) | 67 (23.10) |
| Flexibility (FL) | 11 (3.79) | 123 (42.41) | 156 (53.79) |
| SUBCOMPONENT STRESS MANAGEMENT (ME) | |||
| Stress tolerance (ET) | 2 (0.69) | 204 (70.34) | 84 (28.97) |
| Impulse control (IC) | 1 (0.34) | 24 (8.28) | 265 (91.38) |
| SUBCOMPONENT GENERAL STATE OF MIND (AG) | |||
| Happiness (FAITH) | 34 (11.72) | 212(73.10) | 44 (15.17) |
| Optimism (OP) | 52 (17.93) | 167 (57.59) | 71 (24.48) |
Regarding the BARON Test (emotional intelligence); the mean score for men was 8.66 points higher compared to the mean score for women (354.91 vs. 346.25; p=0.0066). The mean marital status with the highest score was being single 350 points, followed by divorced 349 points (p=0.009). The job position with the highest mean score was physician (373 pts.) followed by nurse (350 pts.) (p=0.0001). With respect to the COPE (coping with stress) test, the marital status with the highest mean score was single (141 points), followed by divorced (140 points) (p=0.0165). The job position with the highest mean score was nurse (144.5 pts.) followed by physician (137 pts.) (p=0.0001) (Table 3).
Table 3. Bivariate analysis of characteristics associated with the BARON test and COPE test
| Features | Baron Test (emotional intelligence) | COPE Test (Coping with stress) | ||
| p-value | p-value | |||
| Sex | 0.0066* | 0.0904* | ||
| Male | 354.91 (57.33) | 135.28 (18.89) | ||
| Female | 346.25 (43.66) | 139.65 (22.97) | ||
| Marital Status | 0.009** | 0.0165** | ||
| Single | 350 (329 - 372) | 141 (132 - 151) | ||
| Partner | 316 (300 - 356.5) | 129 (118 - 143.5) | ||
| Separated | 335.5 (326.5 - 372.5) | 138 (120.5 - 161.5) | ||
| Married | 332 (308 - 359.5) | 128 (114.5 - 154.5) | ||
| Divorced | 349 (336 - 362) | 140 (121 - 159) | ||
| Booth | 0.0001** | 0.0001** | ||
| Dentist | 295 (295 - 295) | 93 (93 - 93) | ||
| Physician | 373 (360 - 388) | 137 (129 - 144) | ||
| Nursing technician | 331 (305 - 365.5) | 129.5 (116 - 145) | ||
| Nurse | 350 (331 - 369) | 144.5 (132 - 169) | ||
| Technologist | 337 (307 - 371) | 136 (130 - 143) | ||
| Type of contract | 0.471* | 0.2306* | ||
| Named | 347.18 (45.31) | 137.44 (23.28) | ||
| CAS | 348.67 (48.11) | 140.54 (21.035) | ||
| Type of work | 0.9476*** | 0.9286*** | ||
| Semi-attendance | 348 (348 - 348) | 44 (51.16) | ||
| On-site | 350 (314 - 371) | 248 (89.86) | ||
(*) Performed with the statistical T student test. (**) Performed with the Kruskal Wallis statistical test. (***) Performed with the Mann-Whitney statistical test.
Significant p-value: p < 0.05
Source: Own elaboration
The correlation was significant between the BARON test and the COPE test, in the population there is a moderate positive monotomic correlation with 0.6003 (p=<0.001). Three strategies of the COPE test were also taken; the planning strategy was found to have a positive monotomic correlation with 0.5271 (p=<0.001), the "positive reinterpretation and growth" strategy was found to have a positive monotomic correlation with 0.5271 (p=<0.001), the "positive reinterpretation and growth.
Planning" was found to have a positive monotomous correlation with a 0.5200 (p=<0.001), and "religious coping" was found to have a positive monotomous correlation with a 0.2051 (p=0.0004) (Figure 1 and Table 4).
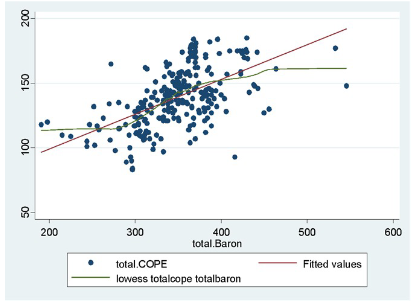
Table 4. Spearman correlation between the BARON test and the COPE test
| Test | Spearman's correlation coefficient | p |
| BARON test | ||
| COPE test | 0.6003 | <0.001* |
| Stress coping strategies | ||
| Planning | 0.5271 | <0.001* |
| Positive reinterpretation and growth | 0.5200 | <0.001* |
| Religious coping *Performed with Spearman's exact test | 0.2051 | 0.0004* |
Source: Own elaboration.
In the simple regression it was found that the average BARON test score increases by 0.269 points for each point increase in the COPE TEST (coef. = 0.269; 95%CI: 0.223 - 0.315). In the multiple regression it was found that the average BARON Test score increases by 0.261 points for each point increase in the COPE TEST (coef. = 0.261; 95%CI: 0.215 - 0.307); adjusted for all covariates of interest (Table 5).
Table 5. Crude and fitted Poisson regression model to evaluate the association between the BARON test and the COPE test
| Charasteristics | Crude analysis | Adjusted analysis | |||||
| coef. | 95% CI | p | coef. | 95% CI | P | ||
| Baron test | 0.269 | 0.223 - 0.315 | <0.001 | 0.261 | 0.215 - 0.307 | <0.001 | |
(*) Adjusted for all variables age, sex, marital status, position, type of contract and type of work. (**) Significant p-value <0.05
PR: Prevalence ratio. 95% CI: 95% confidence interval.
Source: Own elaboration.
DISCUSSION
Main findings
Our results show that emotional intelligence, as measured by the BARON test, correlates moderately positively with stress coping as measured by the COPE test. In addition, emotional intelligence also correlated positively with the three highest scoring emotional coping strategies, which are planning, positive reinterpretation, and religious growth and coping.
Comparison with other studies and Interpretation of results
We found a positive correlation between emotional intelligence and coping to stress, this was similar in a study done in Peru where a correlation coefficient of 0.74 was found.12In another study conducted on students, it was found that there was a correlation between active coping and emotional intelligence.13Understanding the correlation between emotional intelligence and the health and well-being of individuals with stress management generates interest. One possible explanation is a good interaction between health professionals leads to an interpersonal emotional intelligence that leads the individual to ask for help, listen to advice and strategies.14Having coping strategies that seek to regulate emotions generates a cognitive change in the meaning of stressful situations without changing the situation that produces the stress.15In addition, recent research reveals that emotional intelligence of health personnel protects against burnout,16generates commitment to work,17is related to job satisfaction,18well-being,19 20)(21with problem solving and competencies.20)(21Likewise, emotional intelligence also positively influences patient-centered care;22)(23emotionally intelligent health personnel could better cope with work, be more proactive, improving clinical decision making.24
Bar-On demonstrated that emotional intelligence has a significant impact on the capacity for social interaction and stress management.25But the ability to cope with a stressful situation depends on different factors, such as; emotional competence, empathy, self-control and intensity and duration of distress among individuals, gender, wealth level.26In our study we found that the emotional intelligence test increases 0.261 points for each point that the stress coping test increases, this after adjusting for the various factors such as age, sex, marital status, position, type of contract and type of work. One possible explanation would be that stress coping strategies are either adaptive or maladaptive.27This means that stress coping may be influenced by factors specific to the individual such as health status, productivity, personal satisfaction and sociodemographic characteristics.28
Our study also found a significant positive correlation between emotional intelligence and the highest rated stress coping strategies, which were planning, positive reinterpretation, and religious growth and coping; these results are similar to the study done by Marinaki in Greece where a correlation was found between characteristics of emotional intelligence and coping strategies.29In a study of the correlation between emotional intelligence and coping strategies in Nigerian university students, a positive correlation was found between emotional intelligence and stress coping strategies. In addition, students with higher intelligence had a greater ability to cope with stress.30A possible explanation, according to Albesher and Alsaeed, would be that increased emotional intelligence increases the use of positive coping methods, and in turn are instrumental in predicting coping methods in the face of stress.31
Various coping strategies such as meditation, sports, good nutrition, relaxation, humor and leisure activities have been studied to help reduce the effects of stress32. However, coping methods differ according to personality, emotional posture and the individual's interpretation of the situation.(33)In our study the best scoring strategies were planning, positive reinterpretation and growth. These strategies were studied by Cohen which were rational thinking, which would be seen as the positive reinterpretation in a logical way of a stressful situation; individual imagination, which would be understood as future planning and the consequences of the current situation.6There are other very diverse strategies such as those pointed out by Higgins and Endler that are related to orientations that include emotions, avoidance and interactive task performance. the best immediate plan to address the current situation.9For Baqutayan and Mai noted that coping strategies would be the cognitive and behavioral efforts to control, reduce, and maintain externally imposed pressures such as family, friends, work, or college or internal such as emotional conflict, standard setting, or high expectations.10Kim and Han identified that increased emotional control and efficiency help to adapt and practice effective coping strategies to deal with stress.11
LIMITATIONS OF THE STUDY
It is not possible to determine causality or directionality with respect to whether the participants first presented high stress coping and then developed high emotional intelligence, or vice versa. On the other hand, variables that influence stress coping such as lifestyle, IQ, and anxiety level were not taken into account. However, these findings could be useful to understand the picture of stress coping in healthcare workers in a hospital in Lima.
CONLUSIONS
There is a correlation between emotional intelligence and stress coping. In addition, I identified its relationship with stress coping strategies; the strategies that scored highest in the population studied were planning, positive reinterpretation and growth, and religious coping.
Future studies should look for the incidence of emotional intelligence in the decision of the coping strategy to stress, and thus know how this behavior is in health personnel. Therefore, future studies should address the concepts of emotional intelligence and stress with respect to other samples and environments, linking them to different study variables. The application of educational seminar programs and campaigns on the subject should be encouraged among health personnel and thus provide them with tools on emotional intelligence and stress coping strategies
REFERENCES
1. Houtman I, Jettinghof K, Cedillo L, Team WHOO and EH. Sensibilizando sobre el estrés laboral en los países en desarrollo: un riesgo moderno en un ambiente tradicional de trabajo: consejos para empleadores y representantes de los trabajadores [Internet]. Organización Mundial de la Salud; 2008 [citado 19 de noviembre de 2022]. Disponible en: https://apps.who.int/iris/handle/10665/43770 [ Links ]
2. Cortaza Ramírez L, Francisco Torres MD. Estrés laboral en enfermeros de un hospital de Veracruz. México. Rev iberoam educ invest enferm(Internet). 2014;20-6. [ Links ]
3. admin. El 78% de los trabajadores peruanos ha tenido estrés laboral [Internet]. Recursos Humanos, el portal del Capital Humano | Guia empresas recursos humanos peru. [citado 19 de noviembre de 2022]. Disponible en: https://www.infocapitalhumano.pe/recursos-humanos/noticias-y-movidas/el-78-de-los-trabajadores-peruanos-ha-tenido-estres-laboral/ [ Links ]
4. Mayer JD, Caruso DR, Salovey P. Emotional intelligence meets traditional standards for an intelligence. Intelligence. 1999;27(4):267. [ Links ]
5. Scherer KR, Ekman P. Approaches To Emotion. Psychology Press; 2014. 441 p. [ Links ]
6. Cohen RJ. Psychology & adjustment: Values, culture, and change. Allyn & Bacon; 1994. [ Links ]
7. Barreiro Ramos H, Barreiro Peñaranda A, Quesada Soto Z, Fernández Viera E, Marrero Martín O. La responsabilidad profesional del médico. Revista Cubana de Medicina General Integral. abril de 2005;21(1-2). [ Links ]
8. Marquina-Luján RJ. Inteligencia emocional y calidad de vida en personal de salud de cuatro hospitales del sector Público de Lima. Revista Peruana de Obstetricia y Enfermería [Internet]. 21 de septiembre de 2014 [citado 19 de noviembre de 2022];10(2). Disponible en: https://www.aulavirtualusmp.pe/ojs/index.php/rpoe/article/view/719 [ Links ]
9. Higgins JE, Endler NS. Coping, life stress, and psychological and somatic distress. European journal of personality. 1995;9(4):253-70. [ Links ]
10. Baqutayan SMS, Mai MM. Stress, strain and coping mechanisms: An experimental study of fresh college students. Academy of Educational Leadership Journal. 2012;16(1):19. [ Links ]
11. Kim MR, Han SJ. Nursing students' emotional intelligences and coping strategies. Advanced science and technology letters Healthcare and Nursing. 2015;88:53-6. [ Links ]
12. Espino De La Rosa N. "INTELIGENCIA EMOCIONAL Y ESTRATEGIAS DE AFRONTAMIENTO AL ESTRÉS EN ESTUDIANTES DEL QUINTO AÑO DE LA I.E.S. 'MANUEL PRADO' - PUQUIO, 2020". Universidad Autónoma de Ica [cita 12/05/21]; Disponible en: https://renati.sunedu.gob.pe/handle/sunedu/2856192 [ Links ]
13. Fteiha M, Awwad N. Emotional intelligence and its relationship with stress coping style. Health Psychol Open. 6 de noviembre de 2020;7(2):2055102920970416. DOI: 10.1177/2055102920970416 [ Links ]
14. Salovey P, Mayer J. What is emotional intelligence? Emotional development and emotional intelligence: Implications for educators. New York: Basic Books Senge, PM (1998) Sharing knowledge Executive excellence. 1997;15(6):11-2. [ Links ]
15. Shah M, Thingujam NS. Perceived emotional intelligence and ways of coping among students. Journal of the Indian Academy of Applied Psychology. 2008;34(1):83-91. [ Links ]
16. Molero Jurado MDM, Pérez-Fuentes MDC, Gázquez Linares JJG, Simón Márquez MDM, Martos Martínez Á. Burnout Risk and Protection Factors in Certified Nursing Aides. Int J Environ Res Public Health. 30 de mayo de 2018;15(6):E1116. [ Links ]
17. Pérez-Fuentes MDC, Molero Jurado MDM, Gázquez Linares JJ, Oropesa Ruiz NF. The Role of Emotional Intelligence in Engagement in Nurses. Int J Environ Res Public Health. 3 de septiembre de 2018;15(9):E1915. [ Links ]
18. Tagoe T, Quarshie ENB. The relationship between emotional intelligence and job satisfaction among nurses in Accra. Nurs Open. abril de 2017;4(2):84-9. [ Links ]
19. Carvalho VS, Guerrero E, Chambel MJ. Emotional intelligence and health students' well-being: A two-wave study with students of medicine, physiotherapy and nursing. Nurse Educ Today. abril de 2018;63:35-42. [ Links ]
20. Nel JA, Jonker CS, Rabie T. Emotional intelligence and wellness among employees working in the nursing environment. Journal of Psychology in Africa. 2013;23(2):195-203. [ Links ]
21. Por J, Barriball L, Fitzpatrick J, Roberts J. Emotional intelligence: its relationship to stress, coping, well-being and professional performance in nursing students. Nurse Educ Today. noviembre de 2011;31(8):855-60. [ Links ]
22. Sommaruga M, Casu G, Giaquinto F, Gremigni P. Self-perceived provision of patient centered care by healthcare professionals: The role of emotional intelligence and general self-efficacy. Patient Educ Couns. mayo de 2017;100(5):974-80. [ Links ]
23. Snowden A, Stenhouse R, Duers L, Marshall S, Carver F, Brown N, et al. The relationship between emotional intelligence, previous caring experience and successful completion of a pre-registration nursing/midwifery degree. J Adv Nurs. febrero de 2018;74(2):433-42. [ Links ]
24. Kozlowski D, Hutchinson M, Hurley J, Rowley J, Sutherland J. The role of emotion in clinical decision making: an integrative literature review. BMC Med Educ. 15 de diciembre de 2017;17(1):255. [ Links ]
25. Bar-On R. Emotional intelligence: An integral part of positive psychology. South African Journal of Psychology. 2010;40(1):54-62. [ Links ]
26. Brink E. The relationship between occupational stress, emotional intelligence and coping strategies in air traffic controllers [PhD Thesis]. Stellenbosch: University of Stellenbosch; 2009. [ Links ]
27. Perkovic Kovacevic M, Pozgain I, Filakovic P, Grujcic I. Relationship Between Coping Strategies and Emotional Intelligence among Patients with Schizophrenia. Psychiatr Danub. septiembre de 2018;30(3):299-304. [ Links ]
28. Wang Y, Xie G, Cui X. Effects of emotional intelligence and selfleadership on students' coping with stress. Social Behavior and Personality: an international journal. 2016;44(5):853-64. [ Links ]
29. Marinaki M, Antoniou AS, Drosos N. Coping strategies and trait emotional intelligence of academic staff. Psychology. 2017;8(10):1455-70. [ Links ]
30. Aguilar Yuste M. Leadership and Emotional Intelligence during a Crisis. Revista de Relaciones Internacionales, Estrategia y Seguridad. 2021;16(2):47-60. [ Links ]
31. Albesher SA, Alsaeed MH. Emotional intelligence and its relation to coping strategies of stressful life events among a sample of students from the college of basic education in the state of Kuwait. Journal of Educational & Psychological Sciences. 2015;16(04). DOI: http://dx.doi.org/10.12785/JEPS/160409 [ Links ]
32. Ugoji N. Perceived emotional intelligence and stress management among undergraduate students. IFE Psychologia: An International Journal. 2012;20(2):102-6. [ Links ]
33. Borys B, Majkowicz M, Majkowicz H. [Coping with stress in various rescue groups]. Psychiatr Pol. abril de 2003;37(2):337-48. [ Links ]
8Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: April 19, 2023; Accepted: July 17, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
