











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
The revolution in the surgical management of female stress urinary incontinence began with Ulmstein’s report in Europe, 1966, about the tension free vaginal tape technique - TVT, which consisted in placing a sling by the blind passage of a needle through the retropubic space 6.,7.. At the end of the 1990s, this became the most fre- quently performed procedure in the world, with over 500 000 surgeries of this kind and healing rates at 1, 3, 5 and 7 years of 91%, 86%, 87% and 81,3%, respectively(1.-5.).
In France, 2001, Delome presented a variant for this procedure, the transobturator tape - TOT, which consists in placing a suburethral tape through the obturator foramen in the pelvis8.. Ever since, this procedure has been performed thousands of times throughout the world 9.-14..
The TOT technique’s advantages include its sim- plicity and low complication rates. It avoids ab- dominal incisions and passing a needle into the retropubic space, thus decreasing the risk of serious injuries of the bladder, intestine, blood vessels and nerves, rendering the routine use of intraoperative cystoscopy unnecessary 13.-16..
In March 2006, our department decided to apply the TOT technique in patients presenting with stress urinary incontinence who accepted the procedure. Throughout this time, technique-in- herent complications have emerged, so the main author (ASA) proposed avoiding passage of needles through the obturator foramina and cutting the mesh to obtain a smaller tape that would lead to a milder foreign body reaction 17.-19., that is to say, the suburethral tape placing tech- nique (UTP).
We are aware that the American Food and Drug Administration banned the commercialization of mesh for use in pelvic organ prolapse on US territory by a press release on April 16, 2019. However, it only addresses mesh for repair- ing the anterior compartment (cystocele) and the posterior compartment (rectocele), with- out mentioning the sling for the treatment of stress urinary incontinence. Thus, we consider that the technique we present here remains valid.
Methods
We performed an observational comparative study between the UTP and the TOT techniques, where the patients selected for TOT were those operated on the previous shift the same day or the day before the patients operated with the UTP. The study began in January 2012 and patient recruitment stopped in June 2017. Fol- low-up continued until June 2018, with at least one year of follow-up time per patient.
One hundred patients were recruited and ran- domized to undergo voluntarily one of the sur- gical techniques. All patients had a surgical indi- cation for stress urinary incontinence diagnosed via cystometric study with stress test or com- puter-based, and all accepted to participate and signed the informed consent.
We excluded patients diagnosed with urge in- continence or mixed urinary incontinence, with an incomplete preoperative workup, or with contraindications to surgery, as well as patients who did not accept the procedure or had doubts, or who did not sign the informed consent.
The postoperative assessment after discharge was performed two to four weeks after the pro- cedure, with a one-year follow-up consisting in at least two appointments.
Surgical material included a full TOT kit, which consisted in needles for the transobturator pas- sage and a Marlex mesh for the urethra, made of polypropylene or prolene to reduce costs. We obtained four to five tapes out of each Marlex mesh (Figure 1).

Regarding surgical technique, the techniques of TOT and UTP are based on stabilizing the middle area of the urethra by placing a sling. Both tech- niques were performed after vaginal hysterecto- my, if it was required, and/or before finishing the corresponding colpoperineorrhaphy. The TOT technique has been described extensively in the literature 8.-14.,18.
In the case of UTP, the needle does not pass through the obturator foramen. The pubovesical cervical fascia has to be dissected with the fin- ger, until the obturator foramen is reached and the pubic symphysis is touched (Figure 2). The tape is presented, cut and installed with a clamp, after having approximated its position with the finger or the clamp (Figure 3). The same proce- dure is done on the other side (Figure 4).
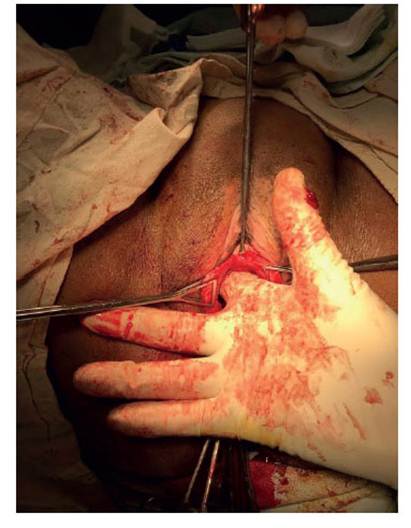
Figure 2 Introducing the index finger to dissect the tissue until it reaches the pubic symphysis, bilaterally. There are no inguinal incisions.


Postoperative management was similar in both techniques. The urinary catheter was retired the day following surgery, coupled with analgesics and antibiotics if required, and the patient was encouraged to walk.
Results
The average age of all patients was 56 years old, and the average parity was five pregnancies (Ta- ble 1). Of the 50 TOT patients, 45 also underwent vaginal hysterectomy and anteroposterior col- poperineorrhaphy, and five had only an antero- posterior colpoperineorrhaphy. Of the 50 UTP patients, 42 also underwent vaginal hysterecto- my and anteroposterior colpoperineorrhaphy, and eight had only an anteroposterior colpoper- ineorrhaphy.
Average time for completion of the TOT tech- nique was 18 minutes and for UTP, 7 minutes (see table).
Complications inherent to the TOT technique were pain in the inguinal area due to Emmet needle puncture, mesh extrusion, wound de- hiscence of anterior colpoperineorrhaphy with mesh exposition and bruising in the left obtura- tor foramen.
There were no complications inherent to the UTP technique (Table 1).
Table 1 Patient characteristics, surgical procedures and complications with the transobturator technique (TOT) and the suburethral tape technique (UTP)
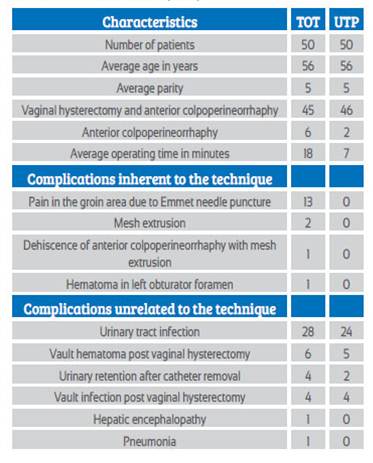
Complications unrelated to the TOT technique were urinary tract infection, vault hematoma af- ter vaginal hysterectomy, urinary retention after removal of urethral catheter (one patient had the catheter replaced once), vault infection after vaginal hysterectomy, hepatic encephalopathy and pneumonia.
Complications unrelated to the UTP technique were urinary tract infection, vault hematoma after vaginal hysterectomy, vault infection after vaginal hysterectomy and urinary retention af- ter removal urethral catheter (Table 1).
Until June 2019, the patients’ evolution and fol- low-ups did not reveal recurrent stress urinary incontinence.
Discussion
We have not found any bibliographic reference describing the suburethral tape placement tech- nique, in our search for comparing it to the TOT technique.
In our study, most patients operated with TOT and UTP had a favorable evolution and early am- bulation after surgery. Both groups had similar age, parity, and underwent similar vaginal proce- dures. However, we observed that the operating time of UTP is shorter than that of TOT: 7 min- utes versus 18 minutes, respectively.
Regarding inherent complications of the TOT technique, we observed pain in the needle punc- ture area, mesh extrusion or rejection, and su- ture dehiscence - both maybe due to foreign body reaction - and local bruising. On the other hand, we did not observe any foreign body com- plications with the UTP technique. This could be due to the shorter and smaller sling it uses, with a smaller area than in TOT.
The TOT kit costs approximately $1000. Mean- while, the value of the suburethral tape is ap- proximately $50 and it is sufficient for four slings for four procedures; this means, each sling has a value of $13.
Regarding complications unrelated to the tech- niques, there were no significant differences.
Finally, we observe that both techniques were effective in the treatment of stress urinary in- continence.
The study’s limitations are that it took place in a public hospital that lacks material resources, and that some patients from both techniques were lost to follow-up because they did not come to their postoperative controls.
We conclude that, in our series, the suburethral tape was better than the TOT because it had a shorter operating time, it had less complica- tions, and it was less expensive.

