










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.23 no.3 Lima jul./set. 2023 Epub 21-Sep-2023
http://dx.doi.org/10.25176/rfmh.v23i3.5670
Clinical Case
Systemic sclerosis sine scleroderma in a woman with centromere antinuclear antibodies, pulmonary and digestive involvement: Case report
1Hospital Víctor Lazarte Echegaray. Trujillo, Perú
2Hospital Edgardo Rebagliati Martins. Lima, Perú
Sine entities are rare in rheumatology. In progressive systemic sclerosis there is a variant of the limited cutaneous form called systemic sclerosis sine scleroderma, whose central feature is the lack of skin involvement, but visceral involvement is present. Positive anti-topoisomerase or anti-centromere antibodies confirm the diagnosis. We present the case of a 63-year-old woman with interstitial lung disease, intestinal transit involvement and Raynaud's phenomenon, with high titers of ANA with a centromeric pattern and positivity for anti-topoisomerase antibodies. When faced with a patient with Raynaud's phenomenon, visceral involvement and elevated ANA, specific antibodies should be requested for the diagnosis of systemic sclerosis in its sine variety.
Keywords: Systemic sclerosis; Raynaud's disease; antinuclear antibodies
INTRODUCTION
In rheumatology, there are few entities with the sine condition (Latin locution meaning "without"); they are rare diseases in which the most florid characteristic that defines the entity is absent; for example, absence of weakness in polymyositis or cutaneous sclerosis in progressive systemic sclerosis (PSS). PSS is a disease in which idiopathic fibrosis is the rule. Its hallmark is skin sclerosis, the presence of which greatly facilitates its rapid and accurate diagnosis. It is classified into limited cutaneous (SSlc), diffuse cutaneous (SSdc), prescleroderma, and systemic sclerosis sine scleroderma (SSss)1. SSss is a rare entity of PSS in its limited variety (2-10% of cases) and is recognized as a variant of PSS, its diagnosis is determined by Raynaud's phenomenon (RyP), visceral involvement and specific antibodies present: Antibodies anticentromeric (AAC) or antitopoisomerase (AAT) antibodies, also called Anti-Scl 70. SSss is a rare entity, diagnosis is usually delayed, a problem that leads to a progression of complications (inexorable advance of pulmonary and digestive involvement). Therefore, in a patient with Raynaud's phenomenon, pulmonary involvement (fibrosis and/or pulmonary hypertension) and involvement of the digestive tract (gastroparesis, gastroesophageal reflux, constipation, dysphagia, heartburn, etc.), AAC or AAT should be investigated to establish the diagnosis of SSss2.
Although it is true, in SSss, there is no skin involvement, this does not differ in the other clinical or laboratory characteristics that may exist, so the prognosis is as similar as in PSS with skin involvement. The treatment of an SSss also does not differ in the classic form of PSS, but the rule is that almost all patients with SSss begin treatment late, when the visceral fibrosis (pulmonary, digestive, renal) has already generated irreversible damage, due to the rarity of this entity3.
The objective and justification of this report is to relate an elevated ANA with a centromeric pattern associated with pulmonary and digestive involvement with a rapid diagnostic suspicion of scleroderma sine scleroderma, a frankly rare entity.
CASE PRESENTATION
A 63-year-old woman, married, housewife, from the Peruvian Amazon. She has no pathological history. The patient denies smoking and alcoholism. Sporadic dry cough began, without fever or weight loss. The cough persisted and became chronic over time. Eight months after the onset of the symptoms, progressive tiredness and fatigue appeared, so she went to the hospital where a physical examination of the respiratory system revealed diffuse velcro-type crackles in the lower 2/3 of both lung fields. The chest X-ray confirmed pulmonary fibrosis, in a ground glass pattern (figure 1).

In addition, the patient begins postprandial discomfort, feeling fullness and dysphagia. There is no variation in appetite. The patient is referred to a national hospital in Lima and a study of the cause of pulmonary fibrosis and dyspepsia begins. In the auxiliary tests, the results are normal, except for high titers of Antinuclear Antibodies (ANA) at 1/5120 with a centromeric pattern. With this result, a study of autoimmune disease was initiated. The physical examination of the abdomen was not contributory. A chest Computed Tomography (CAT) was performed (figure 2) where reticular-type interstitial thickening was reported, predominantly posterobasal subpleural honeycomb-type in the lower 2/3 of the lungs. A walk test was performed, without alterations.
During the hospital stay, Raynaud's phenomenon was verified repeatedly, and no other skin lesions were evident. The patient's hands also did not show distinguishable or characteristic lesions (figure 3). Contrast radiography of the digestive tract was performed (figure 4) and a delay in emptying was demonstrated at higher levels (esophagus and stomach), but no dilatations were seen. He underwent digital capillaroscopy, which revealed splinter hemorrhages in the 3rd finger of the left hand.
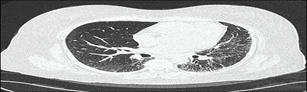
Figure 2. Progressive honeycombing to a subpleural predominance is evidenced, the reason for the tiredness and fatigue in the patient
Given the existing triad (pulmonary fibrosis, digestive involvement and Raynaud's phenomenon), a sine entity is probably diagnosed. A study of antibodies for systemic sclerosis is requested (anti-centromeric antibodies -AAC- and anti-topoisomerase -AAT-). The result showed elevated levels of AAT. It is concluded in a Systemic Sclerosis sine scleroderma (SSss). Treatment was started with azathioprine 100 mg daily, management that causes digestive intolerance, and was changed to mycophenolic acid (MMF) 2 grams daily; In addition, prokinetics are indicated for digestive involvement.

Figure 3. In addition to Raynaud's phenomenon, there was no evidence of proximal or distal skin involvement in both hands
The patient begins progressive improvement of the pulmonary and digestive symptoms. Currently, it is with present progressive improvement. Maintains MMF 1 gram daily and weight gain.

DISCUSSION
Unlike the bibliographic references reviewed (where SSss is classified as a variant of SSlc and positivity necessary for AAC), our patient had SS sine scleroderma, but as a variant of the diffuse cutaneous form, since she presented positivity for AAT and disease. associated pulmonary interstitial4.
Three types of SSss have been proposed: type 1 (total absence of skin involvement), type 2 (absence of skin sclerosis, but presence of telangiectasias, calcifications, or scars) and type 3 (late-onset skin involvement after visceral involvement)5.
The patient started the disease with respiratory symptoms; therefore, it is type 1. Taking into account that there was a delay of approximately two years in the definitive diagnosis of SSss in the patient; said wait agrees with the average time (2.5 + 1.5 years)6.
The immunosuppressant of choice in PSS is methotrexate (MTX), with azathioprine and mycophenolate being valid options. This changes in the SSss, since there is no skin involvement and lung involvement (as was the case with our patient) the drugs of choice are AZA or MMF. In a patient with SSss and general involvement or vital compromise, cyclophosphamide is preferred. Corticosteroids are almost banned in all varieties of PSS (including its sine form)7).
The prognosis of patients with SSss is good (similar to the limited cutaneous form), however, this largely depends on the time it takes to diagnose and the organ affected8.
The patient has pulmonary and digestive interstitial disease, but the good response to MMF favors her and she is considered to have a good prognosis. SSlc also has another rare variety called CREST syndrome, where skin involvement occurs in the form of characteristic calcinosis9.
REFERENCES
1. Chong WH, Saha B, Beegle S. Chronic Dyspnea with Raynaud's Phenomenon and Elevated ANA: A Diagnosis of Systemic Sclerosis Sine Scleroderma. Am J Med Sci. 2022 Mar 8:S0002-9629(22)00098-2. doi: 10.1016/j.amjms.2022.01.023. Epub ahead of print. PMID: 35276077. [ Links ]
2. Alghamdi M, Derbes SJ. Systemic Sclerosis Sine Scleroderma Manifested with Gastrointestinal Bleeding, Antiphospholipid Syndrome and Positive Anti-RNA Polymerase III Antibody: Case Report and Literature Review. Int Med Case Rep J. 2020;13:323-326. https://doi.org/10.2147/IMCRJ.S254859 [ Links ]
3. Adigun R, Goyal A, Hariz A. Systemic Sclerosis. 2022 May 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. PMID: 28613625. [ Links ]
4. Kucharz EJ, Kopec-Medrek M. Systemic sclerosis sine scleroderma. Adv Clin Exp Med. 2017 Aug;26(5):875-880. doi: 10.17219/acem/64334. PMID: 29068586. [ Links ]
5. Hansrivijit P, Omeonu KF, Lawal HO, Gangireddy M, Gadhiya KP, Dhatt RS. A 45-Year-Old Man with Scleroderma Renal Crisis Associated with a History of Systemic Sclerosis Sine Scleroderma. Am J Case Rep. 2020 Nov 24;21:e927030. doi: 10.12659/AJCR.927030. PMID: 33230093; PMCID: PMC7701023. [ Links ]
6. Vera-Lastra O, Sauceda-Casas CA, Domínguez MDPC, Alvarez SAM, Sepulceda-Delgado J. Systemic Sclerosis Sine Scleroderma in Mexican Patients. Case Reports. Reumatol Clin (Engl Ed). 2018 Jul-Aug;14(4):230-232. English, Spanish. doi: 10.1016/j.reuma.2016.11.004. Epub 2017 Jan 3. PMID: 28065485. [ Links ]
7. De Almeida Chaves, S., Porel, T., Mounié, M. et al. Sine scleroderma, limited cutaneous, and diffused cutaneous systemic sclerosis survival and predictors of mortality. Arthritis Res Ther 23, 295. 2021. https://doi.org/10.1186/s13075-021-02672-y [ Links ]
8. de Carvalho, Jozélio Freire MD, PhD; Shoenfeld, Yehuda MD, FRCP, MaACR Systemic Sclerosis Sine Scleroderma After Silicone Breast Implants, JCR: Journal of Clinical Rheumatology: June 2022 - Volume 28 - Issue 4 - p e687-e688 doi: 10.1097/RHU.0000000000001687 [ Links ]
9. Edwards M, Ray J, Al-Taee A, Marsicano E. Systemic Sclerosis Sine Scleroderma as a Rare Etiology of Chronic Intestinal Pseudo-Obstruction. Can Journ Gen Int Med [Internet]. 2021 Sep. 21. doi https://doi.org/10.22374/cjgim.v16i3.494 [ Links ]
8Article published by the Journal of the faculty of Human Medicine of the Ricardo Palma University. It is an open access article, distributed under the terms of the Creatvie Commons license: Creative Commons Attribution 4.0 International, CC BY 4.0 (https://creativecommons.org/licenses/by/1.0/), that allows non-commercial use, distribution and reproduction in any medium, provided that the original work is duly cited. For commercial use, please contact revista.medicina@urp.edu.pe.
Received: June 12, 2023; Accepted: August 12, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
